Secondary Pulmonary Lobule
- What is it?
- The secondary pulmonary lobule is the smallest functional unit of lung structure visible on imaging, typically identified on high-resolution CT (HRCT).
- It is a polygonal unit of lung parenchyma, measuring 1-2.5 cm in diameter, and is composed of multiple acini, which are the smallest functional subunits of the lung.
- Parts:
- Centrilobular Structures:
- A central bronchiole (terminal or respiratory bronchiole).
- A pulmonary artery accompanying the bronchiole.
- Peripheral Structures:
- Interlobular septa, containing pulmonary veins and lymphatics.
- Connective tissue framework forming the boundaries of the lobule.
- Acini:
- Each secondary lobule contains 3 to 25 acini, the basic gas-exchanging units of the lung.
- Centrilobular Structures:
- Size and Shape:
- Approximately 1-2.5 cm in diameter.
- Typically polygonal in cross-section, with a slightly irregular outline.
- Position:
- Distributed throughout the lung parenchyma, with variations in size and density depending on the region of the lung (smaller near the pleura and larger near the hilum).
- Character:
- Defined by its composition of airways, blood vessels, connective tissue, and acini.
- The interlobular septa often appear as thin, linear structures on imaging.
- Blood Supply:
- Arterial:
- A pulmonary artery supplies each centrilobular structure.
- The bronchial arteries contribute to the supporting structures.
- Venous:
- Pulmonary veins drain the periphery via the interlobular septa.
- Arterial:
- Venous Drainage:
- Occurs primarily through the interlobular septa into the pulmonary veins.
- Lymphatic Drainage:
- Lymphatics are present in the interlobular septa and pleural surfaces, draining toward the hilar and mediastinal lymph nodes.
- Nerve Supply:
- Autonomic innervation via the pulmonary plexus.
- Parasympathetic fibers from the vagus nerve and sympathetic fibers from thoracic ganglia.
- Embryology:
- Develops from the pseudoglandular stage (5-17 weeks of gestation), where the bronchial tree and pulmonary vasculature form.
- Applied Anatomy:
- Imaging Application:
- CXR: Secondary pulmonary lobules are not directly visible but are implied through findings like septal thickening in interstitial diseases.
- CT/HRCT:
- The interlobular septa are visible as thin lines in normal lungs.
- Abnormalities include thickening (e.g., pulmonary edema, lymphangitic carcinomatosis), nodularity (e.g., sarcoidosis), or air trapping (e.g., small airway disease).
- Nuclear Medicine: May reveal regional perfusion or ventilation deficits in diseases affecting the lobules.
- Imaging Application:
- Pathological Implications:
- Diseases affecting the secondary lobule can manifest as specific imaging patterns:
- Septal Thickening: Seen in interstitial edema or lymphangitic spread of malignancy.
- Centrilobular Nodules: Common in hypersensitivity pneumonitis or infectious bronchiolitis.
- Ground-Glass Opacities: Indicative of alveolar or interstitial processes.
- Mosaic Attenuation: Reflects air trapping in small airway diseases or vascular pathologies.
- Diseases affecting the secondary lobule can manifest as specific imaging patterns:
- Key Points and Pearls:
- The secondary pulmonary lobule is critical in understanding radiologic patterns of lung diseases.
- Its well-defined boundaries and structures allow for precise localization of pathology on HRCT.
- Variations in size and density reflect regional and pathological differences, aiding diagnosis.
- Parallels with Human Endeavors:
- The secondary pulmonary lobule resembles a well-organized community: each component serves a specialized role (air exchange, circulation, lymphatic drainage) while functioning harmoniously within a defined boundary.
- This parallels urban planning, where infrastructure (roads, utilities) supports specialized zones (residential, industrial) within a city’s framework.
- The meticulous organization of the lobule highlights the balance between complexity and efficiency, a principle echoed in engineering, architecture, and social systems.
A secondary lobule is the smallest functional unit of the lung that
can be seen on high-resolution CT scans. It is a polyhedral structure
measuring about 1-2.5 cm in diameter, surrounded by connective
tissue known as the interlobular septa. Each secondary lobule
contains multiple acini, which are clusters of alveoli where gas
exchange occurs, along with bronchioles, arteries, veins, and
lymphatic vessels. The interlobular septa that define the boundaries
of the secondary lobule contain lymphatic channels and veins,
while the center of the lobule contains the terminal bronchiole and
pulmonary artery. Understanding the anatomy of the secondary
lobule is important in radiology because various interstitial lung
diseases present with characteristic patterns involving these
structures. For example, centrilobular nodules indicate changes
around the bronchioles, while thickened interlobular septa may
suggest conditions like pulmonary edema or lymphangitic
carcinomatosis. Identifying these patterns helps in diagnosing and
differentiating lung diseases.
Parts that Make up the Whole
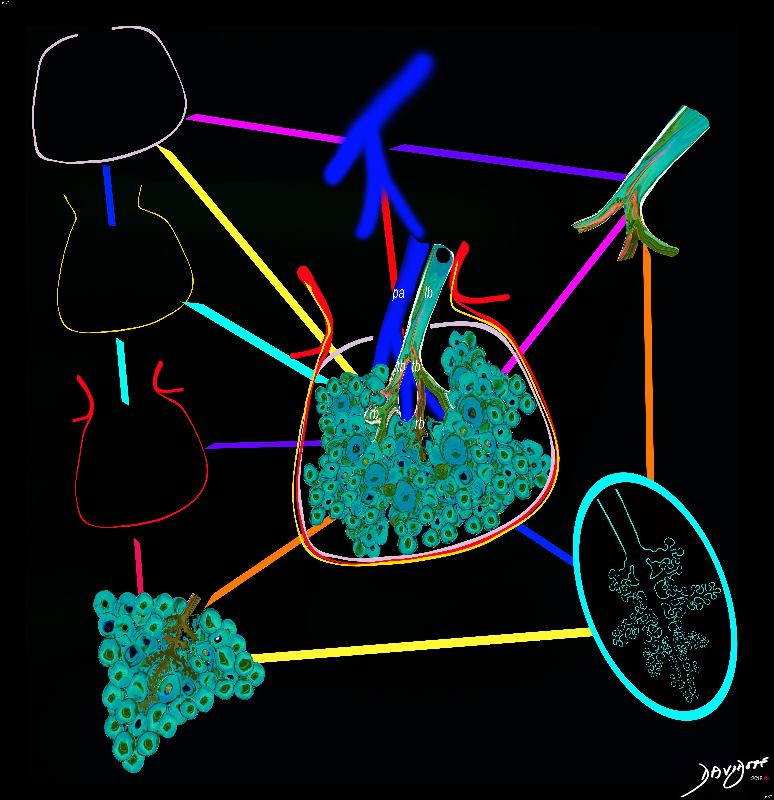
The secondary lobule is housed in a connective tissue framework in which run the lymphatic and venular tributaries . Together these 3 structures form the interlobular septum.
The lobular arteriole enters the framework, accompanied by the lobular bronchiole, and they all run together and form the interlobular septa. This structure measures between .5cms and 2cms and is visible on CT scan.
It is important in clinical radiology since many of the structures can be identified in health, and more particularly in disease, enabling the identification and characterization of many pathological processes.
Courtesy Ashley Davidoff MD The CommonVein.net lungs-0751
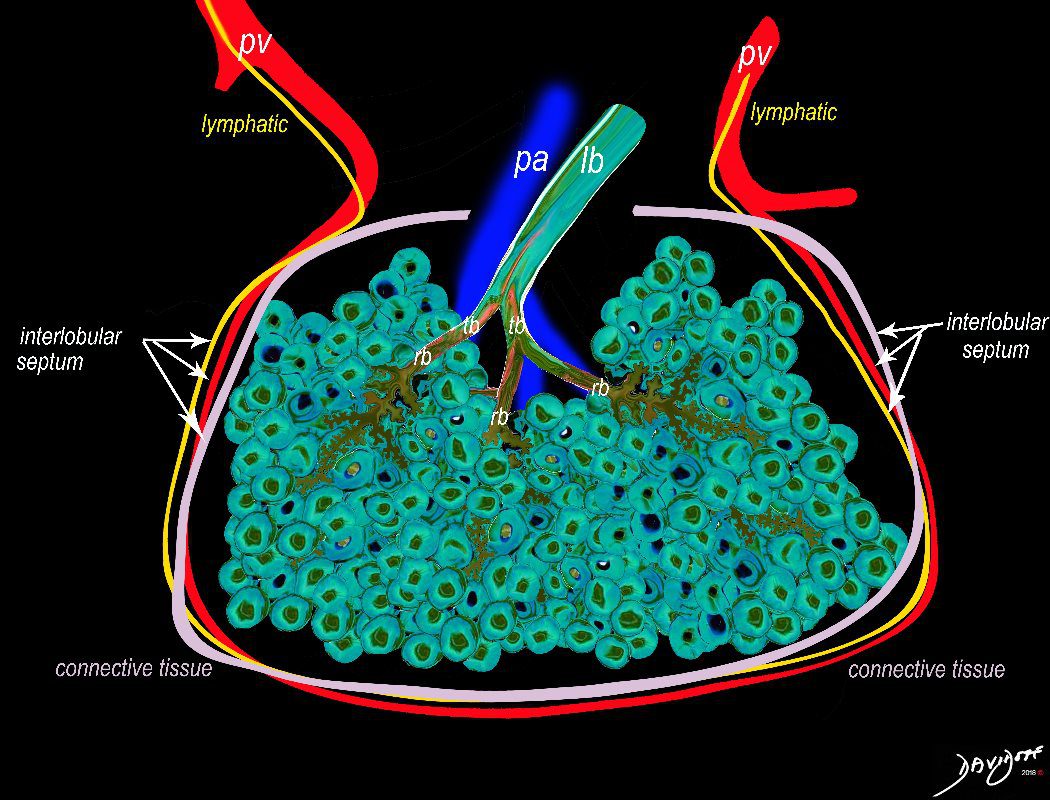
The secondary lobule is housed in a connective tissue framework in which run the lymphatic and venular tributaries . Together these 3 structures form the interlobular septum.
The lobar arteriole enters the framework, accompanied by the lobar bronchiole, and they all run together and form the interlobular septa. This structure measures between .5cms and 2cms and is visible on CT scan.
It is important in clinical radiology since many of the structures can be identified in health, and more particularly in disease, enabling the identification and characterization of many pathological processes.
Courtesy Ashley Davidoff MD The CommonVein.net
lungs-0036-low res
Primary Lobule – Acinus 6-10mm
Distal to the Terminal Bronchiole
Respiratory Bronchiole Onward
3 to 5 terminal bronchioles supplied by a
small bronchus with a diameter of
1 mm (Reid’s lobule) (Reid 1958).
About 12 Acini per Lobule (3-24)
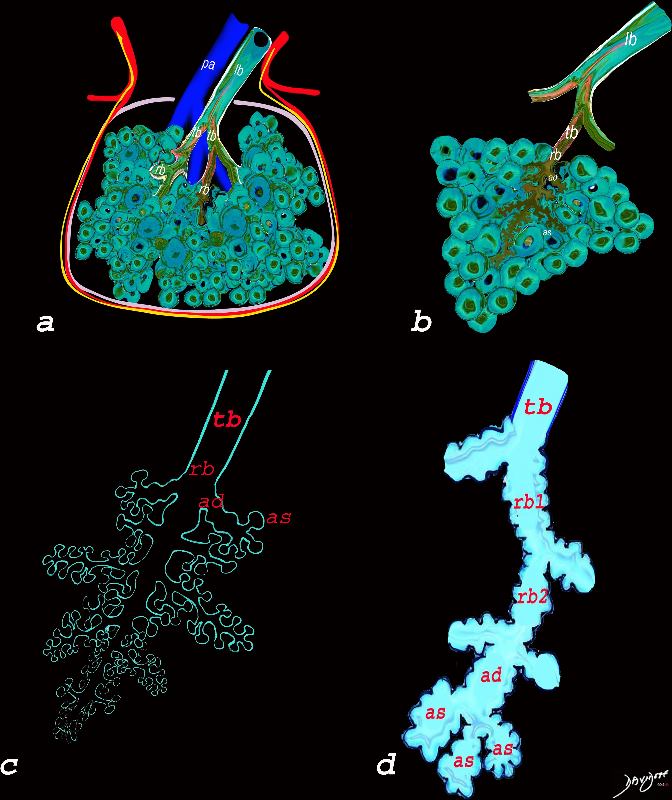
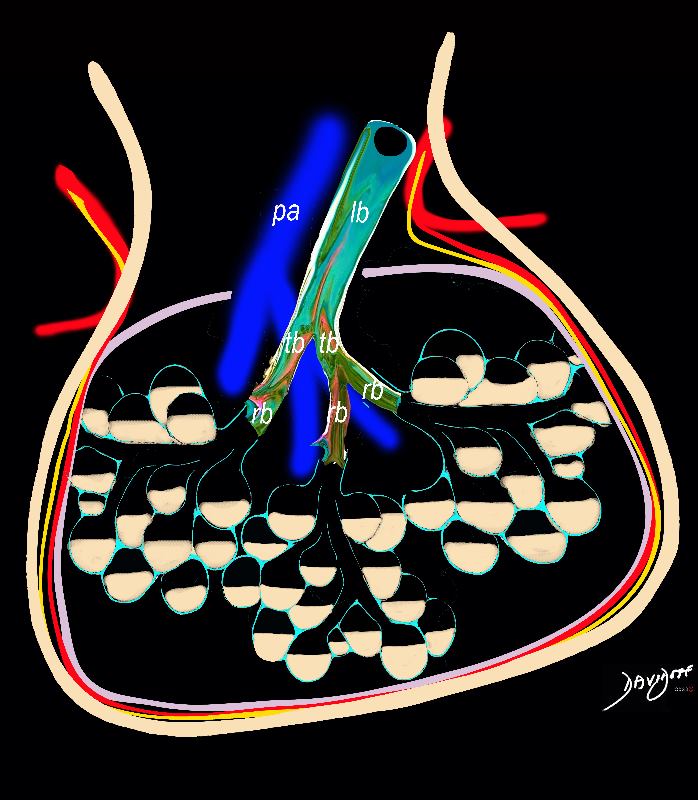
The diagram allows us to understand the the components and the position of the small airways starting in (a) which is a secondary lobule that is fed by a lobular bronchiole(lb) which enters into the secondary lobule and divides into terminal bronchioles (tb) which is the distal part of the conducting airways, and at a diameter of Ashley Davidoff MD TheCommonVein.net lungs-0744
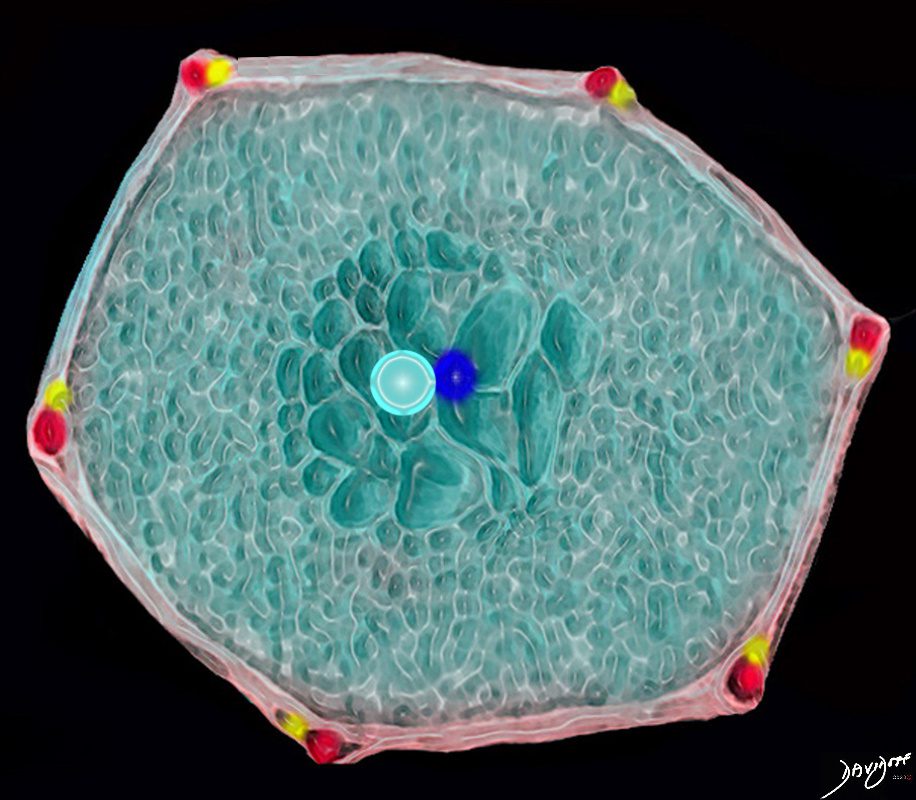
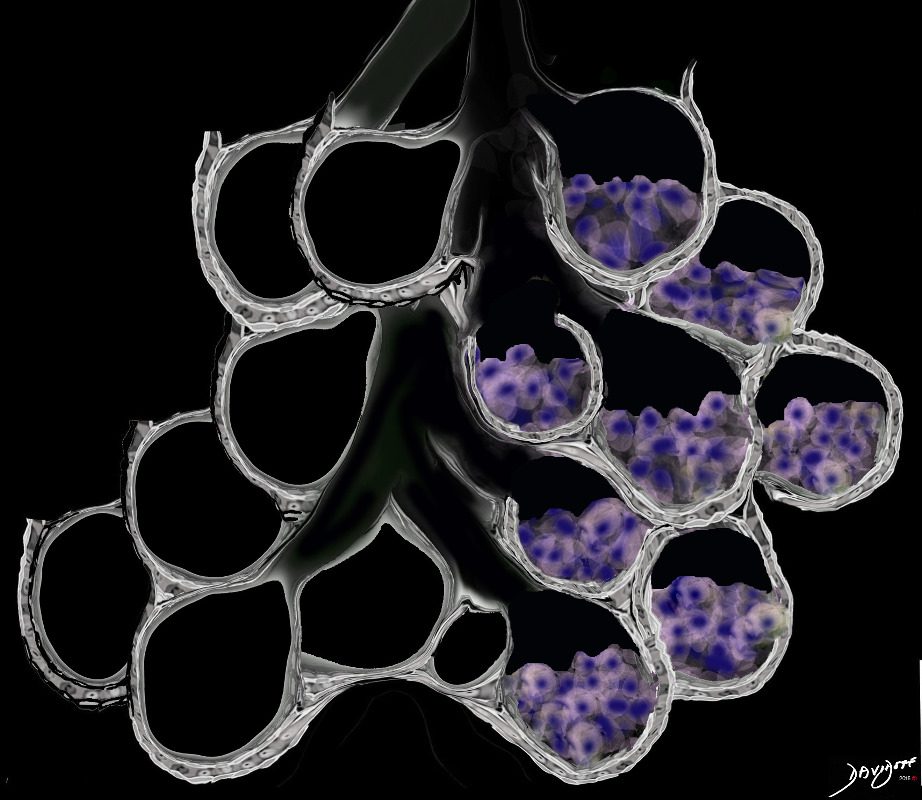
3D image of the polyhedral shaped secondary lobule with a centrilobular bronchovesicular bundle Ashley Davidoff MD. The Common Vein.net lungs-0003
Largest in the Periphery
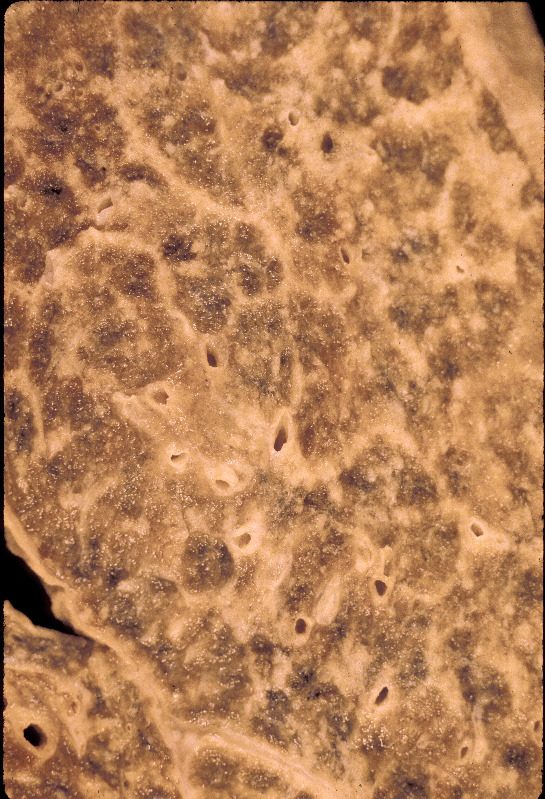
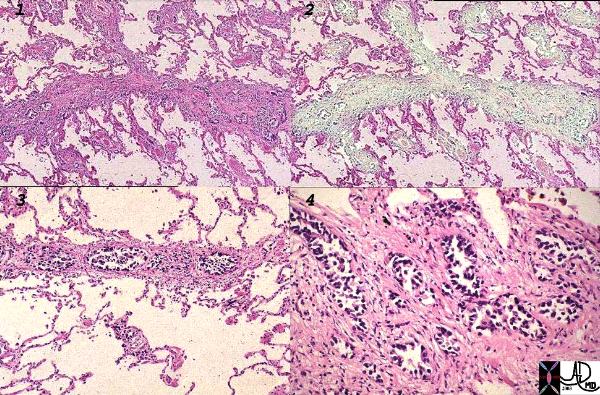
Normal lung histology
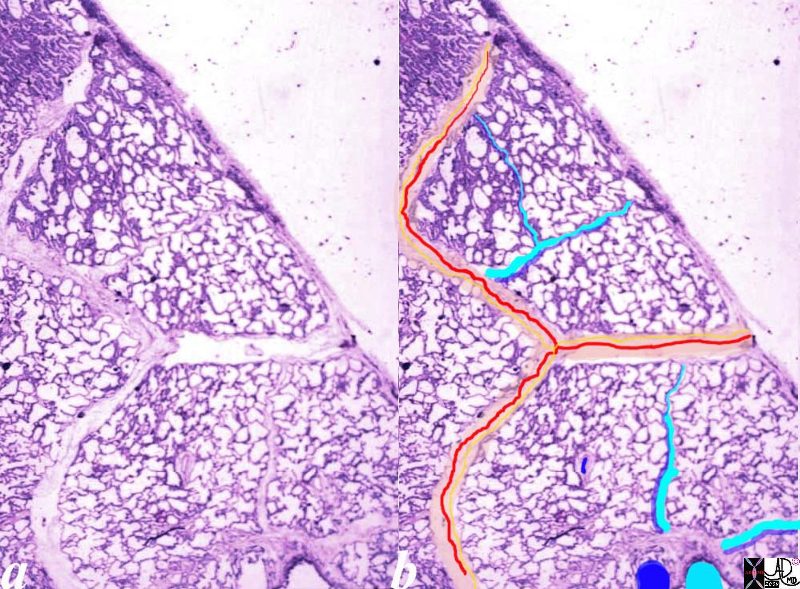
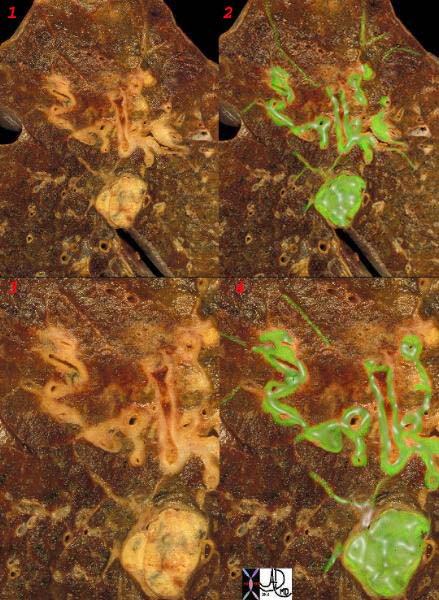
This image is a panoramic view of the lung showing secondary lobules and interlobular septa. Within the interalveolar septae, one sees small venules and lymphatics .
The side by side images show the interlobular septa within which reside the pumonary venules (red) and lymphatics and within the center of the lobule run the respiratory bronchioles (teal) and pulmonary arterioles (blue)
Courtesy Armando Fraire MD. 32649b
key words
lung pulmonary alveoli alveolus secondary lobule interlobular septa vein lymphatic histology
interstitium interstitial
Courtesy of: Armando Fraire, M.D. Ashley Davidoff TheCommonVein.net
32649c06.8s
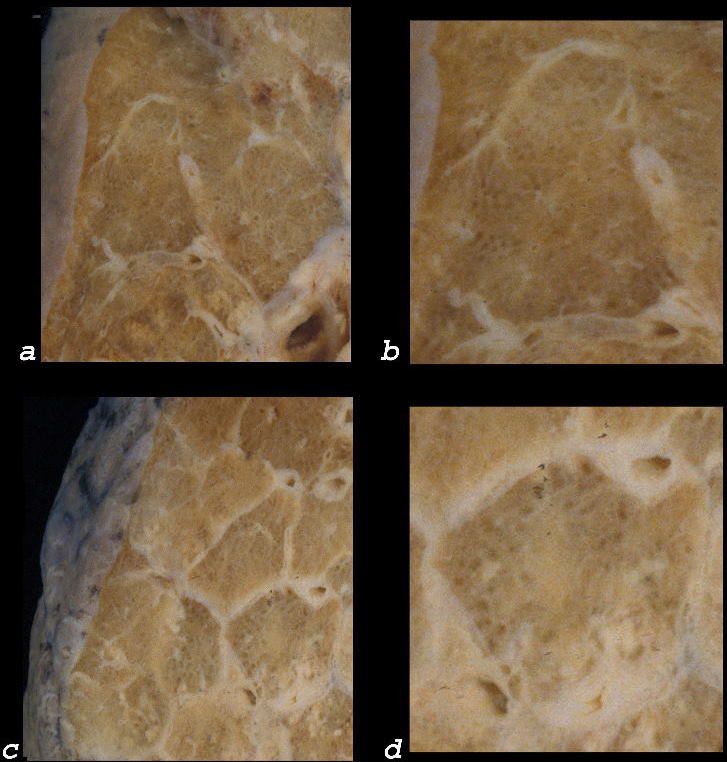
Anatomically
Gross anatomy specimen shows secondary lobules with interlobular septa containing pulmonary venules and the capillary components within the secondary lobules
Davidoff MD TheCommonVein.net 32557bb03.8s
Interlobular Septa
Normal vs Abnormal
Ashley Davidoff MD TheCommonVein.net lungs-0759
Disease
eg Lymphangitis Carcinomatosis
Gross pathology specimen in the coronal plane of the right lung shows extensive irregular thickening of the interlobular septa secondary to lung cancer and lymphangitis carcinomatosis
Ashley Davidoff MD TheCommonVein.net 32327.8
Secondary Lobule in CHF
Varied Sizes and Shapes
Periphery vs Centrally
Tend to be a Paucity Posteriorly
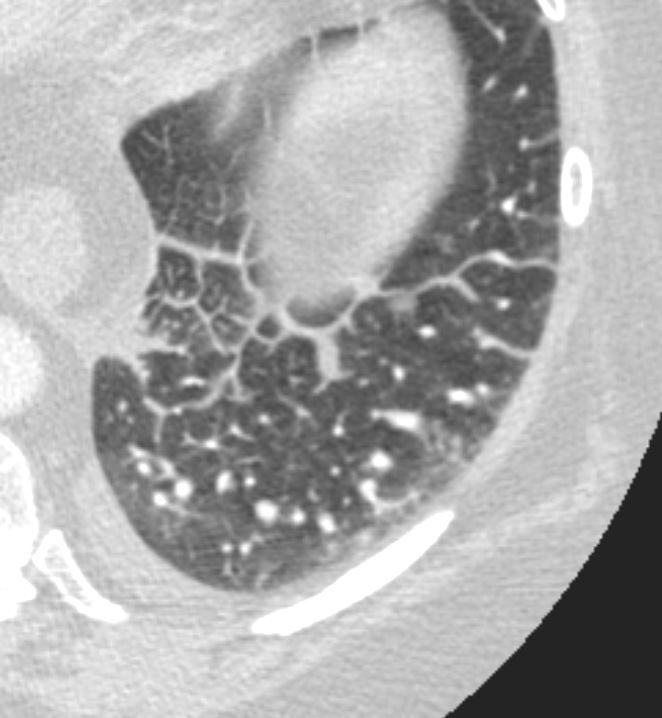
Axial CT in a patient with CHF demonstrates the heterogeneous morphology of the secondary lobule. In this patient the lobules in the periphery are larger than the centrally placed secondary lobules. In addition the peripheral lobules are more rectangular and those centrally are more of a polyhedral shape.
Ashley Davidoff MD TheCommonVein.net 135831
Small Peripheral Secondary Lobules and Varying Shapes Centrally
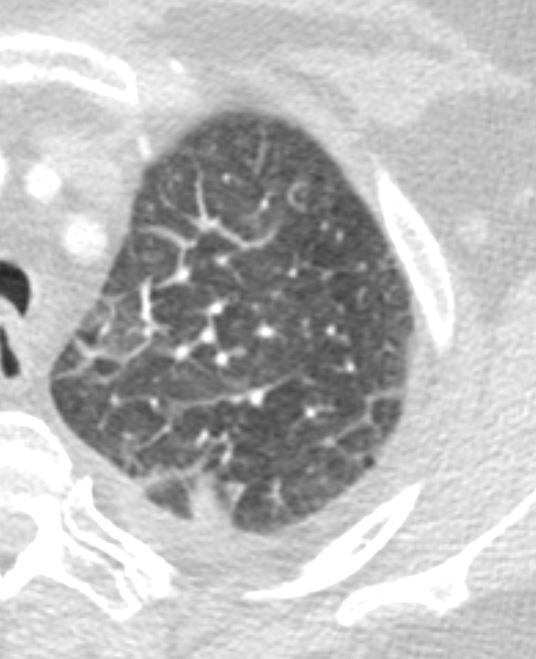
Axial CT in a patient with CHF demonstrates the heterogeneous morphology of the secondary lobule. In this patient the lobules in the periphery are smaller than the centrally placed secondary lobules. In addition the central lobules are more irregular in shape and are hexagonal or polygonal.. There is a small effusion.
Ashley Davidoff MD TheCommonVein.net 135834
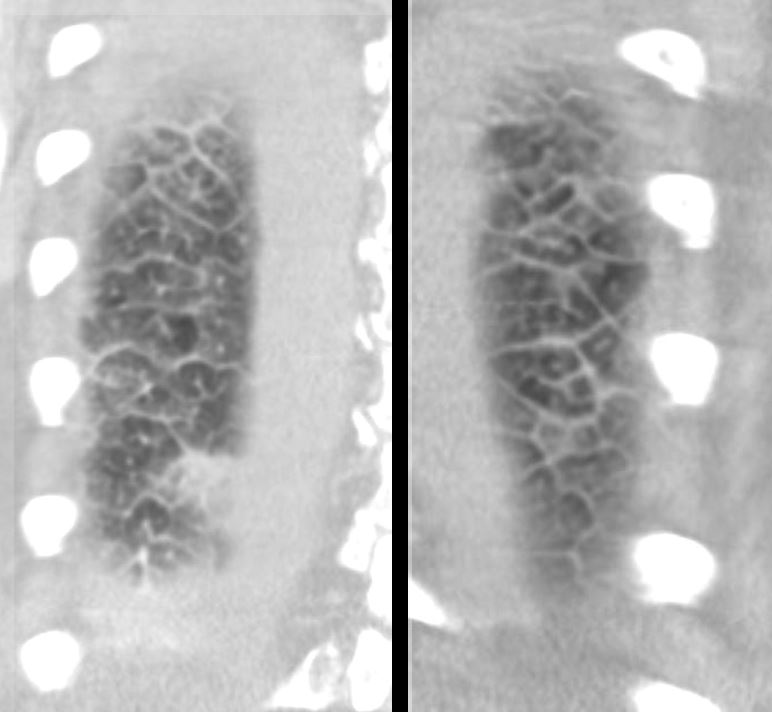
Coronal CT through the posterior chest in a patient with CHF demonstrates the heterogeneous morphology of the secondary lobule. There is a wide range of sizes and shapes, with wide variations of hexagonal and polygonal morphology. Some of the shapes are innate but consideration must be given to the orientation of the lobule and the varying angles we may catch them in a single plane of this technique.
Ashley Davidoff MD TheCommonVein.net 135832c
Depends on Its Orientation in Various Parts of the Lung and
How You Cut it on CT
Centrilobular Structures
Entering Small Airways and Arteries
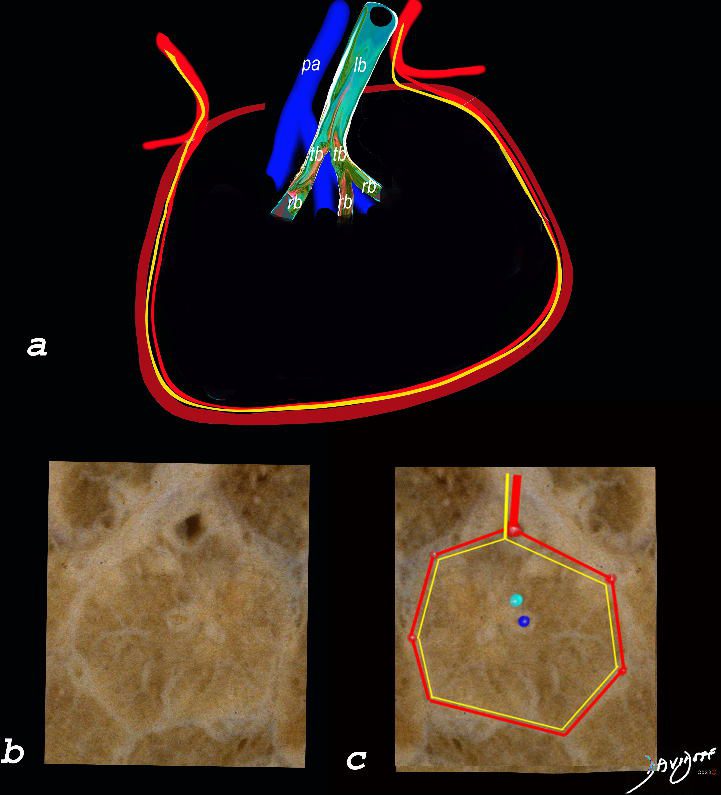
The top image (a) shows an anatomic drawing of a secondary lobule of the lung subtended by a lobular bronchiole (lb) and arteriole (pa). The interlobular septum contains the venule (red) lymphatic (yellow) and septum (maroon)
The anatomical specimen of the lung (b) shows normal intralobular parenchyma while image c shows the centrilobular arteriole (navy blue) and centrilobular bronchiole (teal) and interlobular venule (red) and lymphatics (yellow) The interlobular septum is slightly thickened
Ashley Davidoff TheCommonVein.net
Lymphatics Around The Bronchovascular Bundle
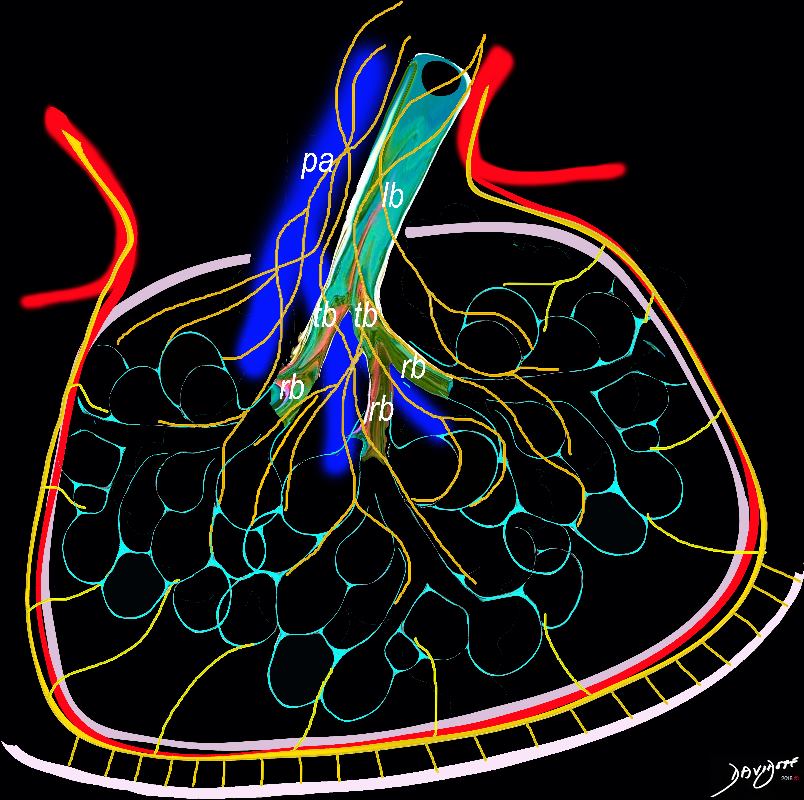
The diagram shows the 2 systems of lymphatic drainage at the level of the secondary lobule. The superficial system drains some of the interstitium of the secondary lobule, runs in the interlobular septa and drains all the pleura. Thee pathway to the lymph nodes in the mediastinum is via the pulmonary veins. The deeper system drains the interstitium in the interalveolar septa, and then they travel along the bronchovascular bundle accompanying the bronchi and pulmonary artery and into the lymph nodes of the hila and mediastinum
Ashley Davidoff MD TheCommonVein.net lungs-0768
Radiology Peripheral Secondary Lobule
Relatively Large and Often Rectangular 1-2.5cms
Centrilobular Arteriole and Bronchiole 1mm
Wall of Terminal Bronchiole .1mm (below res of CT)
Wall of Acinar or Respiratory Bronchiole .05mm
Interlobular Septum measure .1mm (100 μm)
CT Spatial Resolution,
in the range of
0.5 to 1.0 mm
Therefore under normal circumstance
We are able to visualize a
1mm centrilobular arteriole
But not
a 1-mm bronchiole
with wall thickness measures approximately 0.15 mm;
Nor
Interlobular Septum (.1mm)
Ashley Davidoff MD
47152c01
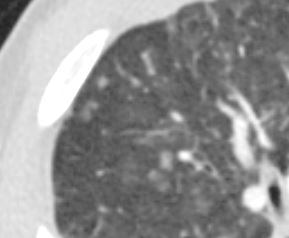
Centrilobular Arteriole and Bronchiole CHF
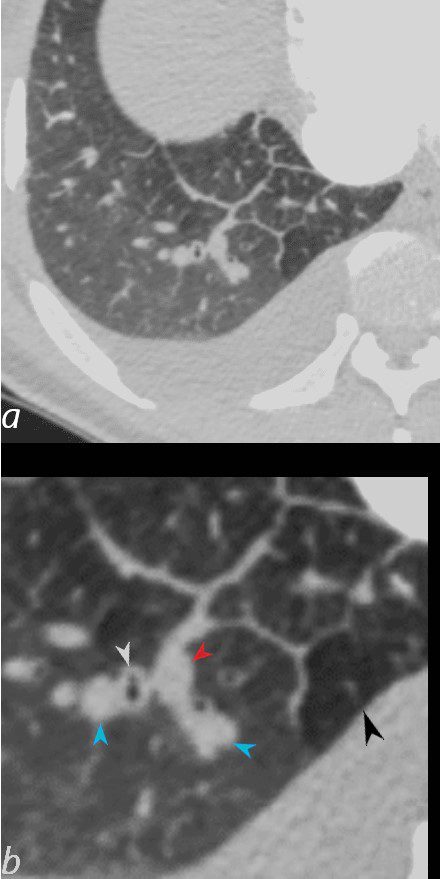
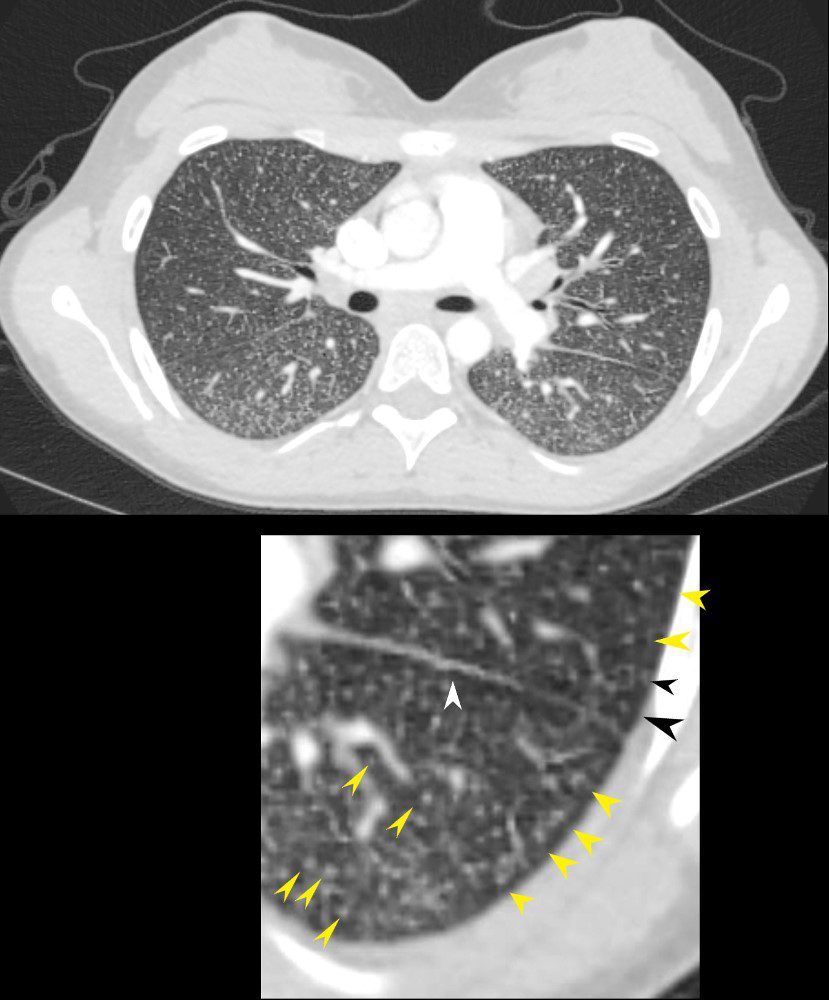
50-year-old female with diabetes, chronic renal failure and congestive heart failure. CT in the axial plane through the right posterior recess, shows thickened interlobular septa at the right base, congested arterioles (light blue arrowheads, b), alongside the bronchioles, peribronchial cuffing (white arrowheads, b), a congested pulmonary venule in the interlobular septum (red arrowhead arrowheads, b), ground glass changes and a secondary lobule demonstrating mosaic attenuation (black arrowhead arrowheads, b). The IVC is dilated and a small complex effusion is present.
Ashley Davidoff MD TheCommonvein.net 135783cL 193Lu
Centrilobular Nodules From Volume Overload
Pre Dialysis 3 days earlier
Ground Glass Changes Kerley B Lines Centrilobular Nodular Congestion
Ground Glass Changes Kerley B Lines Centrilobular Nodular Congestion
Ashley Davidoff MD TheCommonVein.net 04
Ground Glass Changes Significantly Improved, Kerley B Lines and Centrilobular Congestion Resolved with Possible Mosaic Attenuation and Mosaic Attenuation
Ashley Davidoff MD TheCommonVein.net 04
Airways
This drawing shows a secondary lobule with centrally located dilated airspaces starting with the respiratory bronchiole and extending to the proximal structures including the alveolar ducts, sacs and alveoli
Ashley Davidoff TheCommonVein.net
Ashley Davidoff MD
TheCommonVein.net lungs-0038
The red arrows point to the soft tissues of the centrilobular emphysema consisting of the arterioles and bronchiolar walls (not usually visible.
71-year-old female presents with history emphysema
Chest X-ray shows hyperinflated lungs with flattened hemidiaphragms and increase in the retrosternal space and right ventricular enlargement based on the decrease in the retrosternal air space
CT scan confirms the presence of centrilobular emphysema, predominantly in the upper lobes with associated right atrial, right ventricular and pulmonary arterial enlargement. The LA and LV are normal
These findings are consistent with cor pulmonale and pulmonary hypertension, secondary to emphysema.
Ashley Davidoff MD
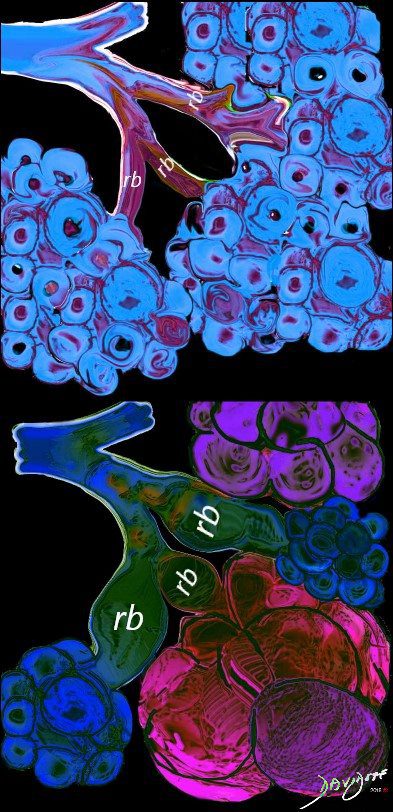
Small Airway
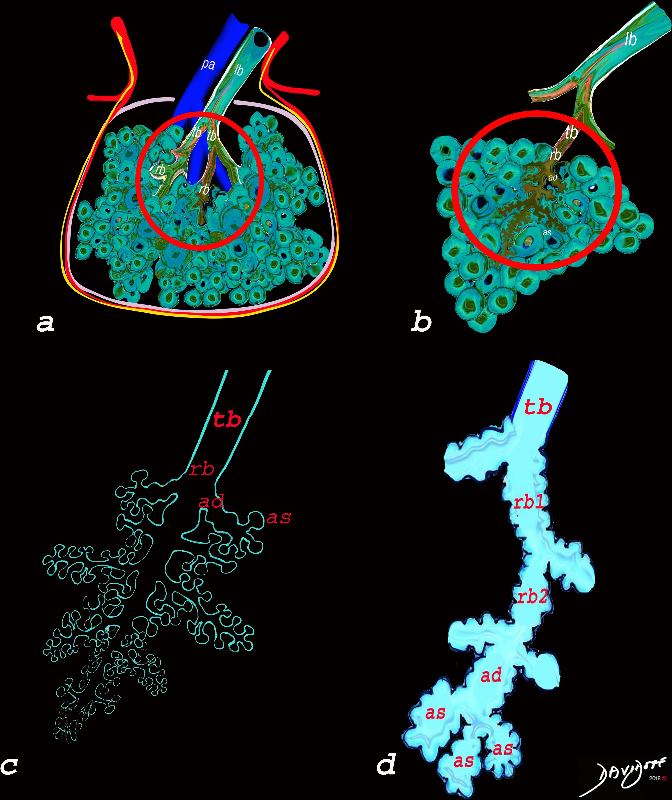
The diagram allows us to understand the the components and the position of the small airways starting in (a) which is a secondary lobule that is fed by a lobular bronchiole(lb) which enters into the secondary lobule and divides into terminal bronchioles (tb) which is the distal part of the conducting airways, and at a diameter of 2mm or less . It divides into the respiratory bronchiole (rb) a transitional airway which then advances into the alveolar ducts(ad) and alveolar sacs (as) Diseases isolated to the small airways do not affect the alveoli and hence there is peripheral sparing Ashley Davidoff MD TheCommonVein.net lungs-0749
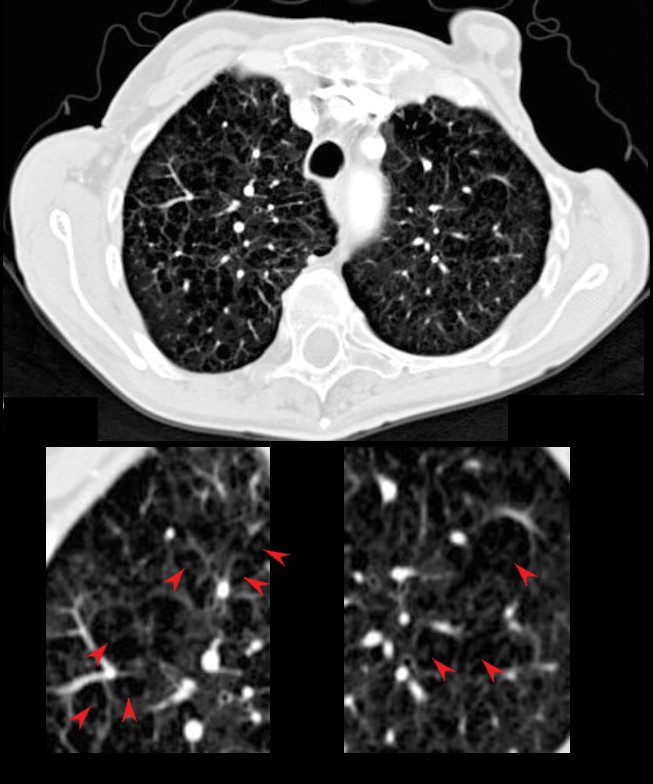
Tree in Bud Centrilobular Nodules Mosaic Attenuation
TB Tree in Bud
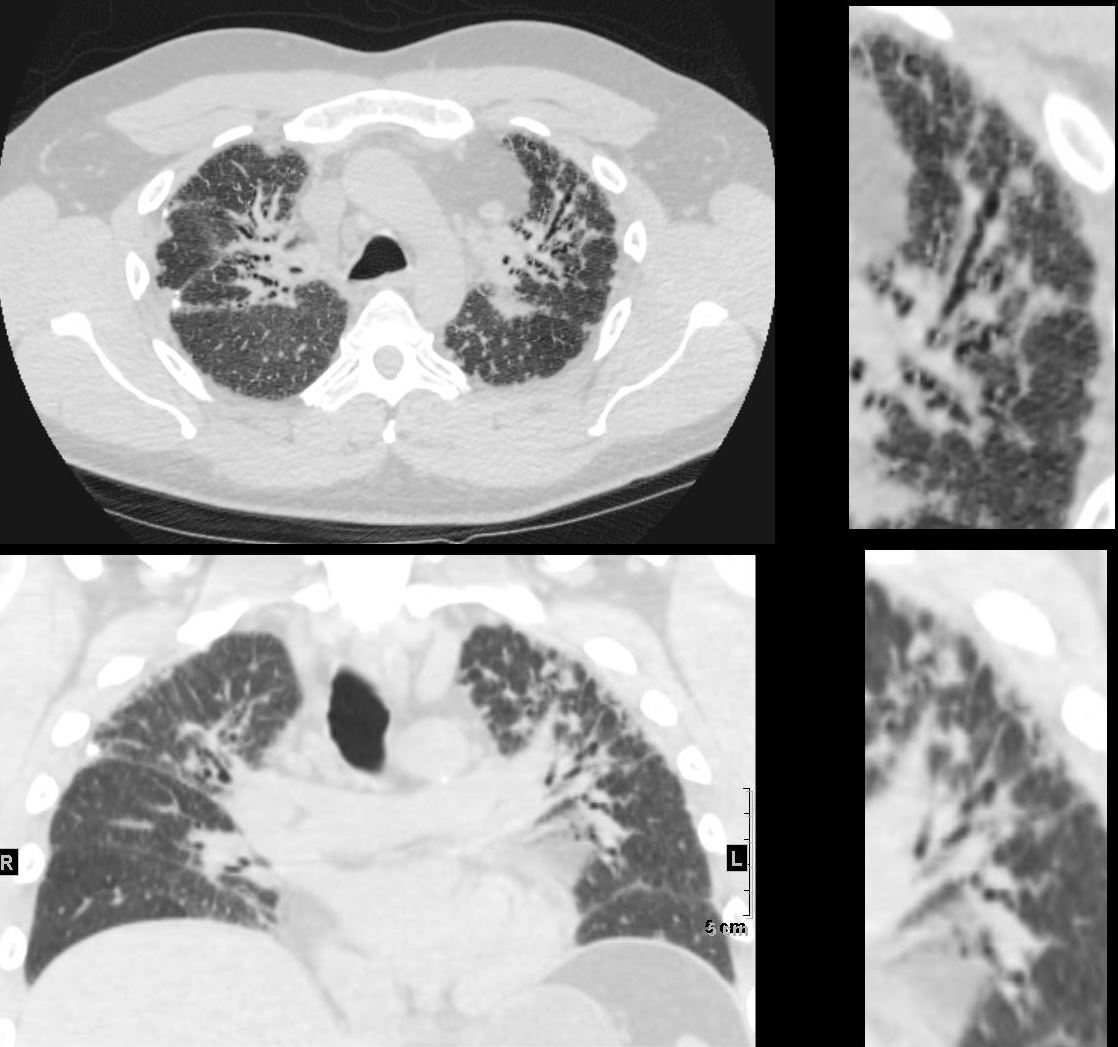
39-year-old immigrant Vietnamese male presents night sweats fever and cough. CT in the axial plane through the mid chest shows innumerable micronodules resulting from transbronchial spread with resultant tree in bud pattern scattered through the right lung (magnified in the right lower image). There are minimal similar changes in the lingula (magnified left lower image)..
Ashley Davidoff MD TheCommonvein.net 135789c 006Lu
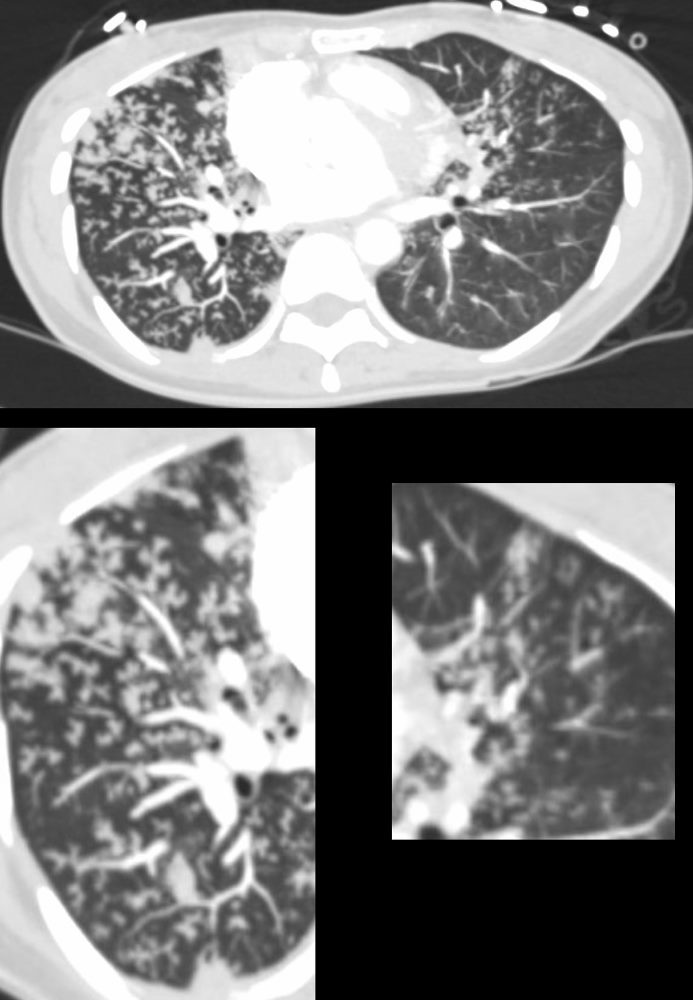
Allergic Bronchopulmonary Aspergillosis (ABPA) Bronchitis and Bronchiectasis
60 year old male with history of asthma, allergic bronchopulmonary aspergillosis (ABPA)
CT scan shows left upper lobe bronchiectasis and soft tissue/fluid impaction in the anterior segmental and subsegmental airways associated with tree in bud appearance (yellow arrowhead) and centrilobular nodules (red arrowhead) reminiscent of associated small airway disease
Ashley Davidoff TheCommonVein.net
Aspiration
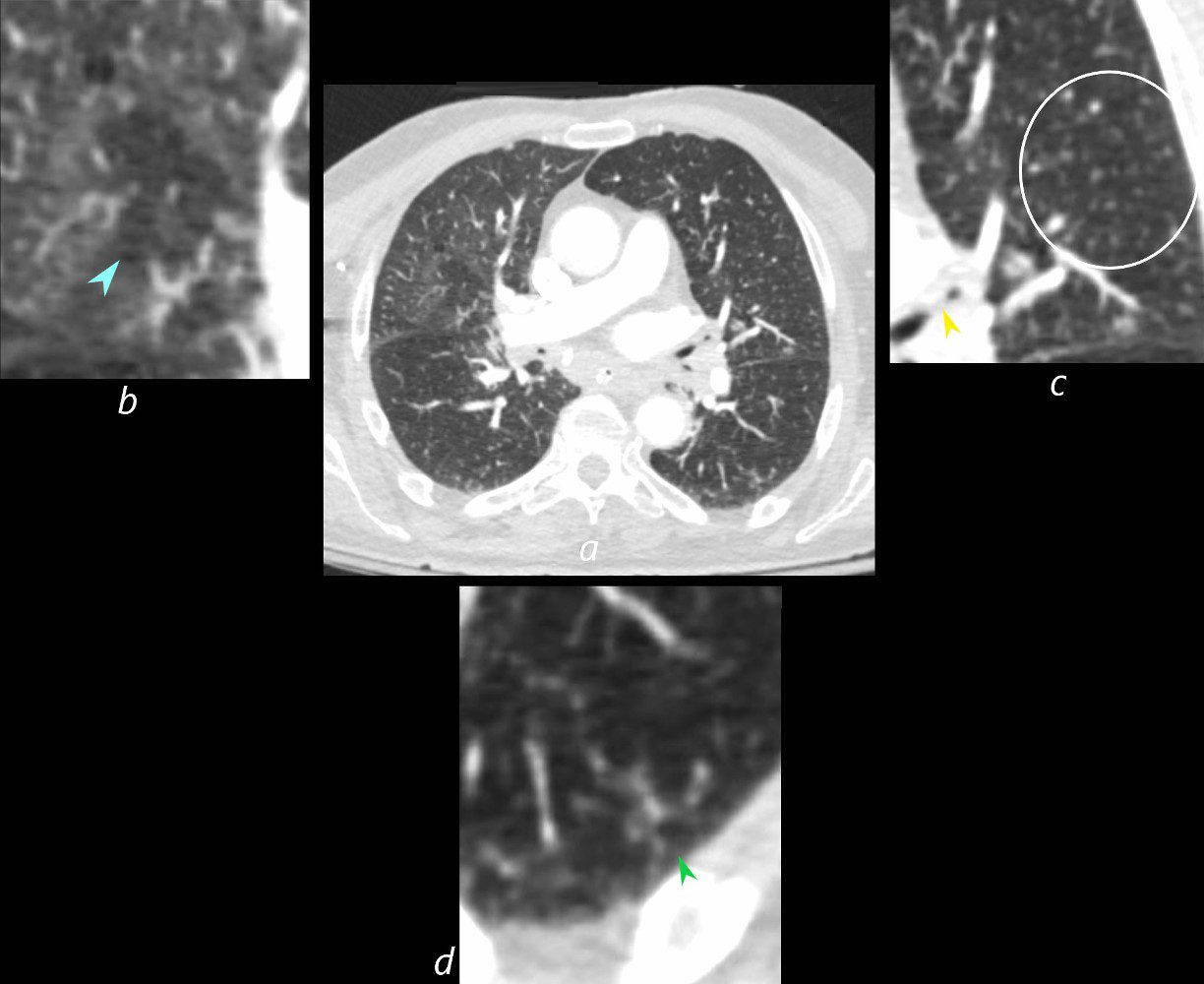
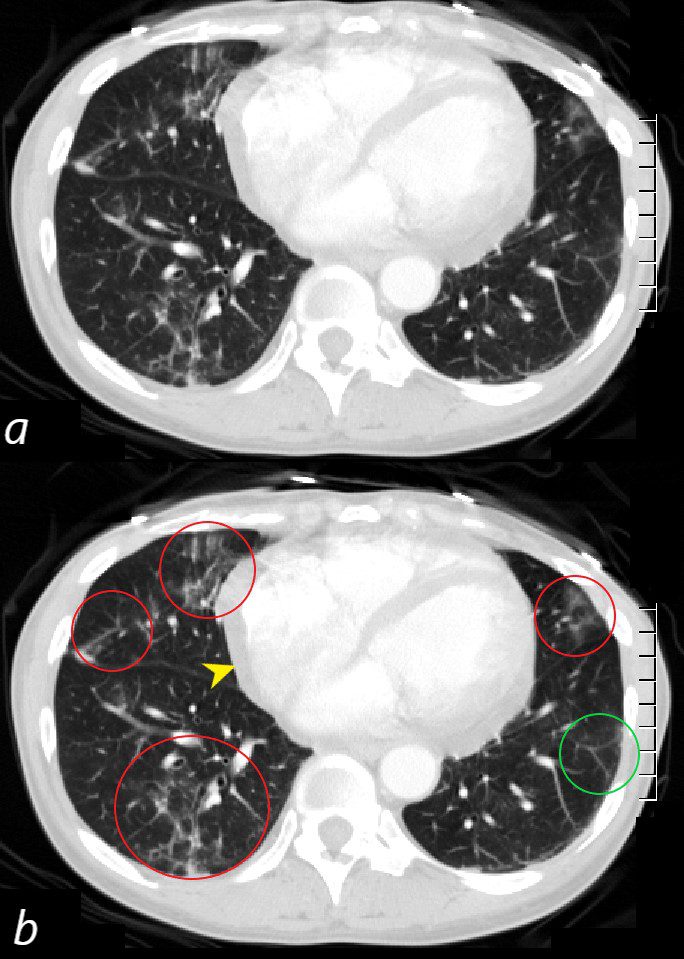
73-year-old man presents with respiratory difficulty following trauma and difficult placement of a nasogastric tube. CT scan through the upper chest at the level of the right pulmonary artery shows a focus of mosaic attenuation in the right upper lobe with a central vasoconstricted vessel (b blue arrowhead). The left upper lobe bronchus contains aspirated material (c yellow arrowhead) and there are multiple ill-defined micronodules (b, white circle). The left lower lobe shows peripheral tree in bud nodularity (d green arrowhead). In the clinical context of technical difficulty with a recently placed NG tube acute, aspiration of fluid gastric content with small airway involvement is a diagnostic consideration despite the lack of alveolar changes
Ashley Davidoff MD TheCommonVein.net 135762cL
Centrilobular Nodules
Miliary Histoplasmosis
22-year-old female presents with flu like symptoms
CT of the chest at the level of the main pulmonary artery shows extensive diffuse miliary disease. Some of the nodules are centrilobular (yellow arrowheads). Some of the secondary lobules suggest mosaic attenuation (black arrowhead). The nodular and irregular appearance on the fissure (white arrowhead) indicates peri-lymphatic distribution.
Ashley Davidoff MD TheCommonvein.net 131708cL
Smokers Bronchiolitis
CT in the axial plane of a chronic cigarette smoker shows multiple ill defined ground glass micronodules dominantly in the upper lobes. Within the right upper lobe there are 2 bronchovascular bundles showing ground glass appearance to the subsegmental airway .
Ashley Davidoff MD TheCommonVein.net 135844
Hypersensitivity Pneumonitis
Ashley Davidoff MD TheCommonvein.net lungs-0732b01
Ashley Davidoff MD TheCommonVein.net lungs-0722
Ashley Davidoff MD TheCommonVein.net lungs-0729
Ashley Davidoff MD TheCommonVein.net lungs-0731
HP Mosaic Attenuation Centrilobular Nodules Air Trapping Head Cheese Sign
55-year-old female with shortness of breath. She keeps birds for pets Axial CT through the mid lung fields on inspiration (upper image) shows diffuse ground glass changes with low attenuation regions Expiration images (below)shows increase in the density of this region indicating that this region is normal lung
Ashley Davidoff MD TheCommonVein.net 13554
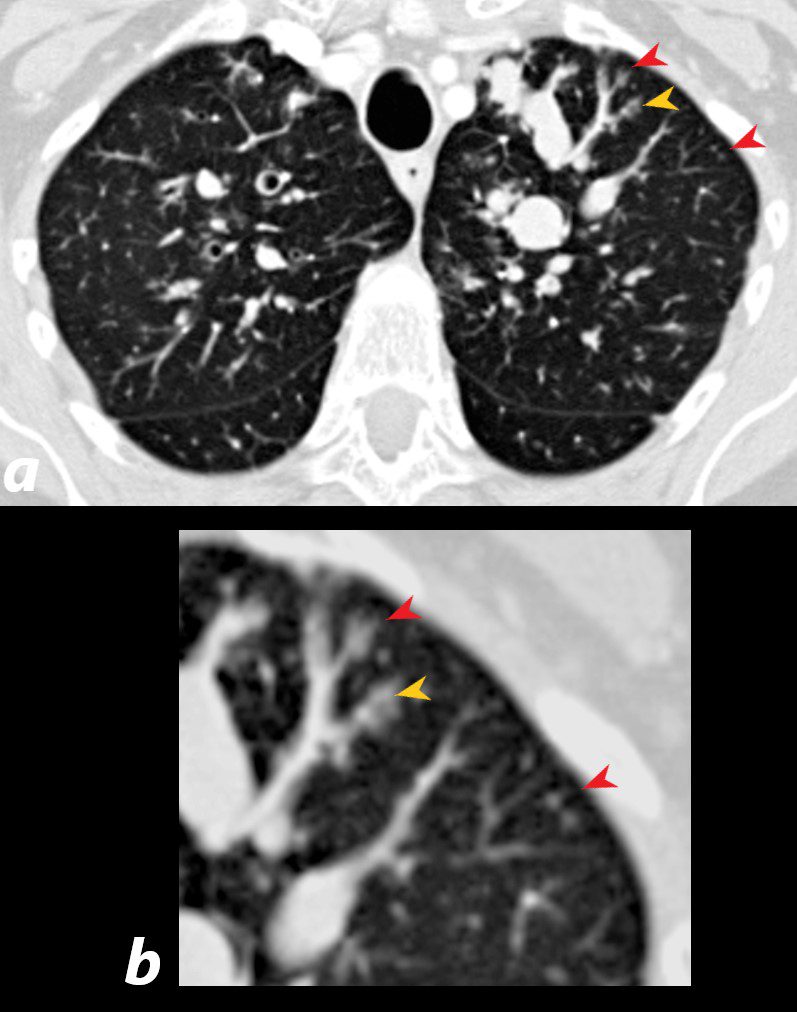
Hypersensitivity Pneumonitis Centrilobular Nodules
CT in the axial (upper)and coronal plane (lower panels) show most prominent and progressive changes in the anterior segment of the left upper lobe
The findings are characterized and by evidence of thickening of the bronchovascular bundle (upper right panel) and centrilobular nodules (lower right panel) indicating small airway disease
Ashley Davidoff MD TheCommonVein.net 135839
Acute Eosinophilic Pneumonia
Small Airway Involvement
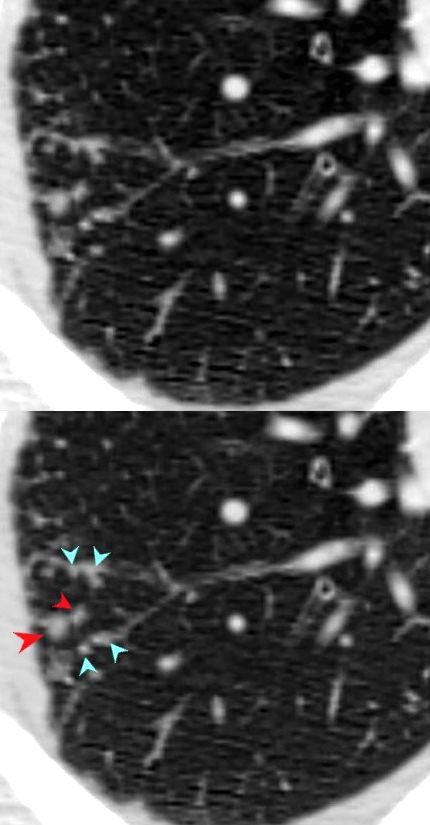
Small Airways Infiltration with Eosinophils and Inflammatory Exudate – Centrilobular Nodules
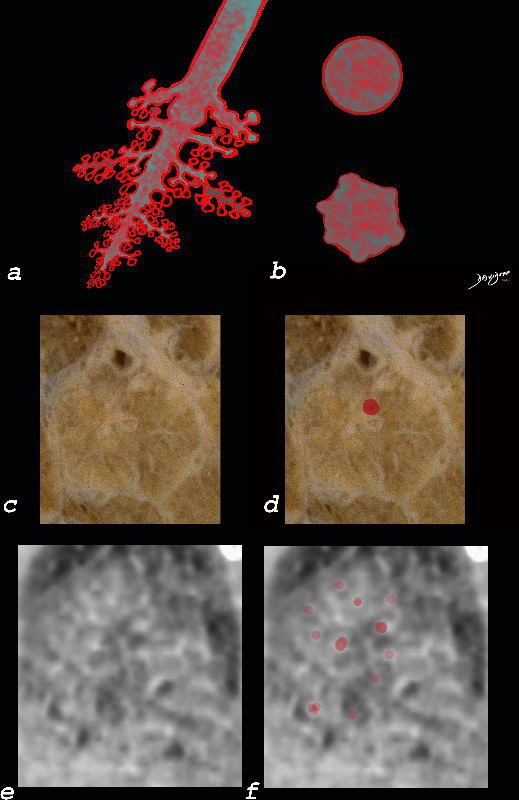
The diagram shows the small airways of the lung including the respiratory bronchiole, alveolar ducts and alveolar sacs in coronal (a) and in cross section (b) and correlated with an anatomic specimen of a secondary lobule that contains a thickened interlobular septum . The respiratory bronchiole is overlaid in maroon (d), next to the arteriole. Images e and f are magnified views of a CT of the lungs in a patient with acute eosinophilic pneumonia and the centrilobular nodules reflecting small airway disease are highlighted in f.
Ashley Davidoff MD The CommonVein.net lungs-0760b
Acute Eosinophilic Pneumonia
Alveolar
Interstitial
Interlobular Septal Involvement
Alveolar and Interalveolar Interstitial Infiltration with Eosinophils and Inflammatory Exudate – Ground Glass Changes
The ground glass changes are a combination of the cellular and exudative inflammatory response in the small airways, alveoli, interalveolar septa and interstitium, and thickened alveolar septum
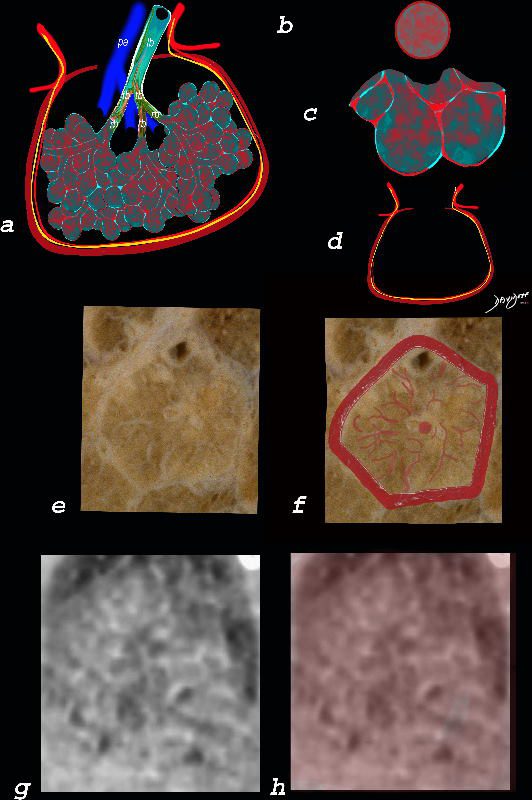
The diagram shows the abnormal secondary lobule (a) The involved components include the small airways(b) alveoli and interalveolar interstitium (c) and the thickened interlobular septum (d) surrounding the secondary lobule due to an inflammatory process, cellular infiltrate and congestion of the venules and lymphatics in the septum. An anatomic specimen of a secondary lobule from a patient with thickened interlobular septa and interstitial thickening is shown in image e, and is overlaid in red (f) . A magnified view of an axial CT of the lungs in a patient with acute eosinophilic pneumonia shows thickened interlobular septa and centrilobular nodules (g) The inflammatory changes in the aforementioned structures result in an overall increase in density of the lung manifesting as ground glass changes (g) and overlaid in red (h)
Ashley Davidoff MD The CommonVein.net lungs-0762
If the Alveoli Get Too Full
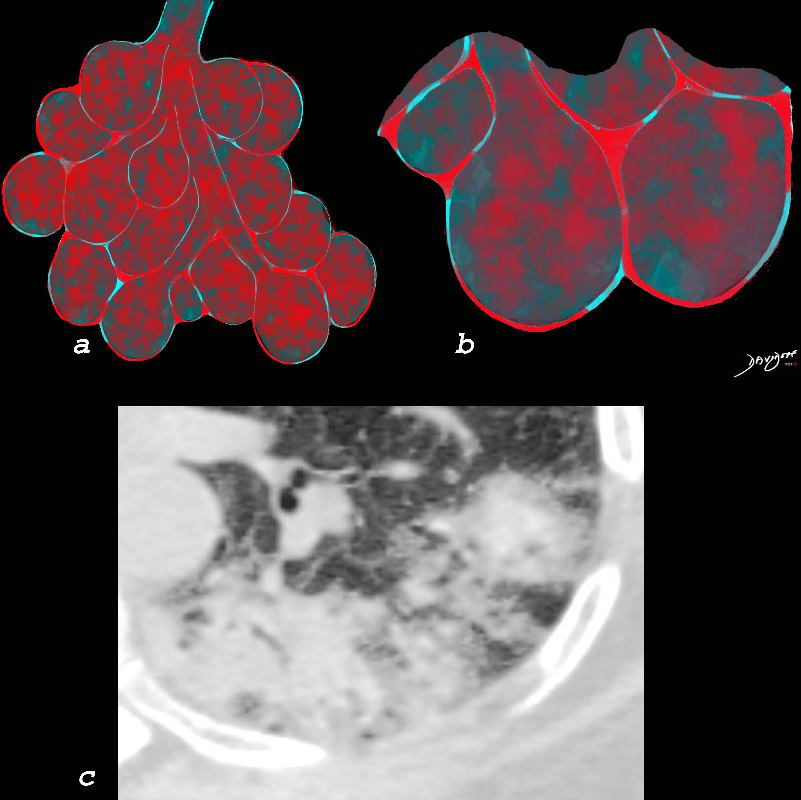
Chronic eosinophilia is characterised by alveolar filling with eosinophils and inflammatory exudates(a) and interalveolar interstitial thickening, (overlaid in red in b). The infiltrates are classically peripherally positioned, usually upper lobes, more commonly bilateral but can be unilateral, and manifest as consolidation and or ground glass opacities. The CT shows a peripheral consolidation in the left upper lobe
Ashley Davidoff MD The CommonVein.net lungs-0764
Distribution
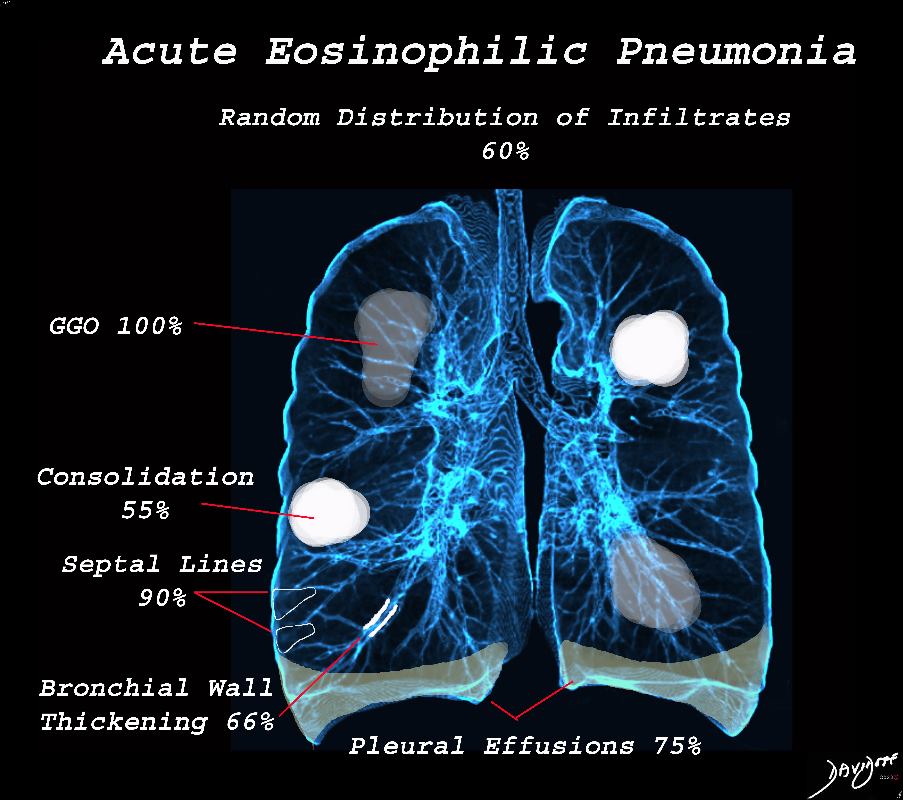
Acute Eosinophilic pneumonia is characterised by ground glass opacities (100%) and sometimes consolidation (55%) most commonly with a random distribution 60%. Septal lines (90%) and thickening of the bronchovascular bundles (66%) and bilateral pleural effusions (75%) were common.
Ashley Davidoff MD TheCommonvein.net lungs-0775-bL (Reference De Giacomi F et al)
Chronic Eosinophilic Pneumonia Affects the
Alveoli and
Alveolar Septal Interstitium
Chronic eosinophilia is characterised by alveolar filling with eosinophils and inflammatory exudates(a) and interalveolar interstitial thickening, (overlaid in red in b). The infiltrates are classically peripherally positioned, usually upper lobes, more commonly bilateral but can be unilateral, and manifest as consolidation and or ground glass opacities. The CT shows a peripheral consolidation in the left upper lobe
Ashley Davidoff MD The CommonVein.net lungs-0764

Chronic eosinophilia is characterised by alveolar filling with eosinophils and inflammatory exudates(a) and interalveolar interstitial thickening, (overlaid in red in b). The infiltrates are classically peripherally positioned, usually upper lobes, more commonly bilateral but can be unilateral, and manifest as consolidation and or ground glass opacities. The CT shows bilateral peripheral consolidations in the upper lobes
Ashley Davidoff MD The CommonVein.net lungs-0775e

Chronic eosinophilia is characterised by alveolar filling with eosinophils and inflammatory exudates(a) and interalveolar interstitial thickening, (overlaid in red in b). The infiltrates are classically peripherally positioned, usually upper lobes, more commonly bilateral but can be unilateral, and manifest as consolidation and or ground glass opacities. The CT shows bilateral peripheral consolidations in the upper lobes
Ashley Davidoff MD The CommonVein.net lungs-0775-e
CT scan in the coronal performed 6 months ago at the time of clinical presentation shows upper lobe predominant peripheral infiltrates more prominent in the left upper lobe. Subsequent diagnosis by BAL of chronic eosinophilic pneumonia (CEP) was made
Ashley Davidoff TheCommonVein.net
Lymphatics
Central Zone
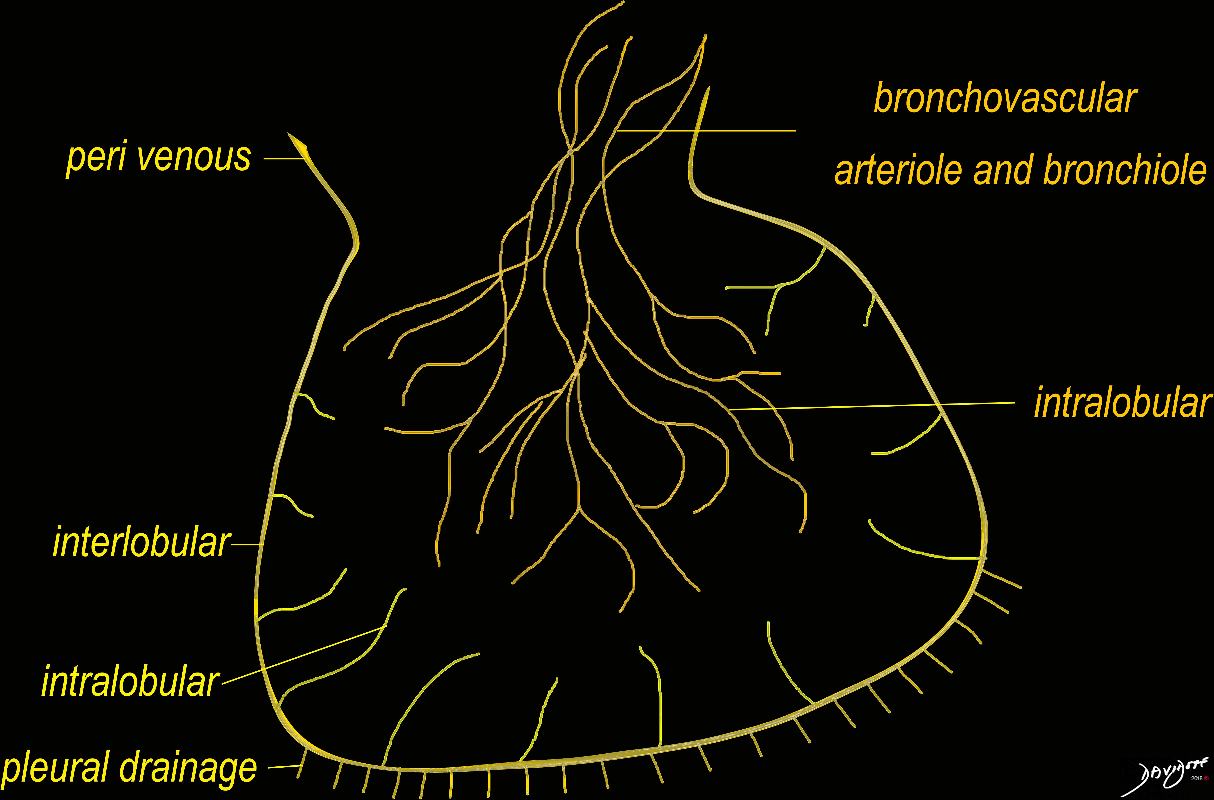
The diagram shows the 2 systems of lymphatic drainage at the level of the secondary lobule. The superficial system drains some of the interstitium of the secondary lobule, runs in the interlobular septa and drains all the pleura. Thee pathway to the lymph nodes in the mediastinum is via the pulmonary veins. The deeper system drains the interstitium in the interalveolar septa, and then they travel along the bronchovascular bundle accompanying the bronchi and pulmonary artery and into the lymph nodes of the hila and mediastinum
Ashley Davidoff MD TheCommonVein.net lungs-0767
SARCOIDOSIS, ACTIVE – ALVEOLAR FORM
SARCOIDOSIS, ACTIVE – ALVEOLAR FORM
48-year-old previously well presented with dyspnea and initial CXR showed an infiltrate at the right base, and clinically resolved. He presented a year later with right chest pain and low grade ever and the CXR showed patchy opacities in the LUL and in the RLL
A subsequent CT showed LUL nodular opacities and subpleural rim of consolidation in the LUL and more prominently at both lung bases, associated with significant mediastinal adenopathy. Lympho-vascular nodularity was noted in the bronchovascular bundles as well as in the interlobular septa, consistent with sarcoidosis
CXR and CT 4 years later showed almost complete resolution of the parenchymal findings and the CT findings except for minimal reticulation and scarring in the subpleural regions
Ashley Davidoff MD
Intralobular Parenchyma
The Secondary Lobule is a Microcosm of the Lung
Ground Glass
art
Focal Intralobular Disease

GGO in the secondary lobule reflects alveolar process and is one of the presenting appearances of unifocal or multifocal BAC. It is a slow growing in situ disease that may not change in size over two years but continued surveillance is necessary.
Courtesy Ashley Davidoff MD
TheCommonVein.net 45465b01
The Cup Half Full with Cellular Elements
Gray rather than Black or White
Ground Glass Opacity (GGO) Caused by Cellular Accumulation with Partial Filling of the Alveolus Ground glass opacification may be caused by partial filling of the alveolus with cellular material with partial replacement of air with solid material with the net density being gray rather than white if the alveolus were fully filled. The black of the airway nor the white of the vessels may blend with the gray density and hence they are not visualized in ground glass opacities.
Ashley Davidoff MD TheCommonVein.net lungs-0707a
Diffuse Intralobular Ground Glass Changes of the Secondary Lobule
The Cup Half Filled With Fluid
Ashley Davidoff TheCommonVein.net lungs-0738b
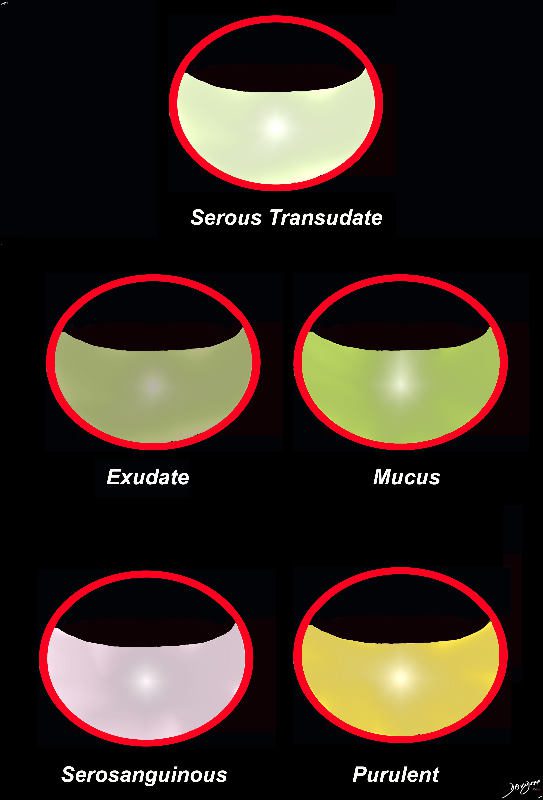
The acute inflammatory process results in fluid exudation into the alveoli which can take the form of a serous transudate, and exudate or in the form of mucus, and when severe (eg ARDS) can result in tissue and vessel destruction and could be be blood tinged. Infected fluid could be mucoid or purulent. The extent of filling the alveoli results either in a ground glass appearance when partially filled or a consolidation when filled.
Ashley Davidoff MD TheCommonVein.net
lungs-0701
Alveolar Septal Amyloidosis
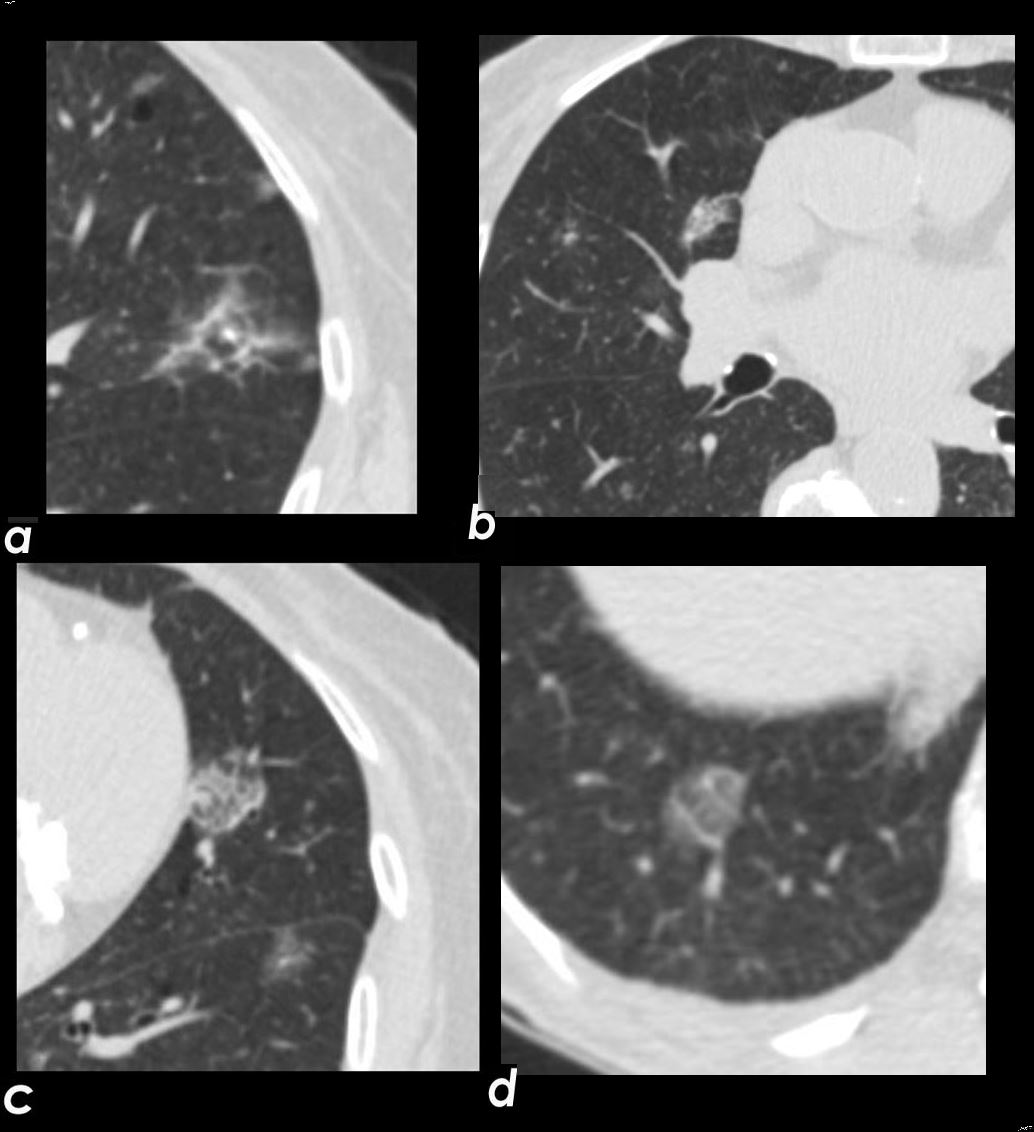
Axial CT images through the chest exemplifies the diffuse alveolar-septal amyloidosis at its mildest and earliest form
Image a, shows a secondary lobule with thickened interlobular septa with a centrilobular nodule either reflecting peribronchial or periarteriole involvement. Image b shows a mixed nodule likely reflecting intralobular alveolar involvement. Images c and d show thickened interlobular septa and a reticular intralobular ground glass abnormality pattern each with a centrilobular nodule
Ashley Davidoff Boston Medical Center TheCommonvein.net LV-005 c01
CHF and The Secondary Lobule
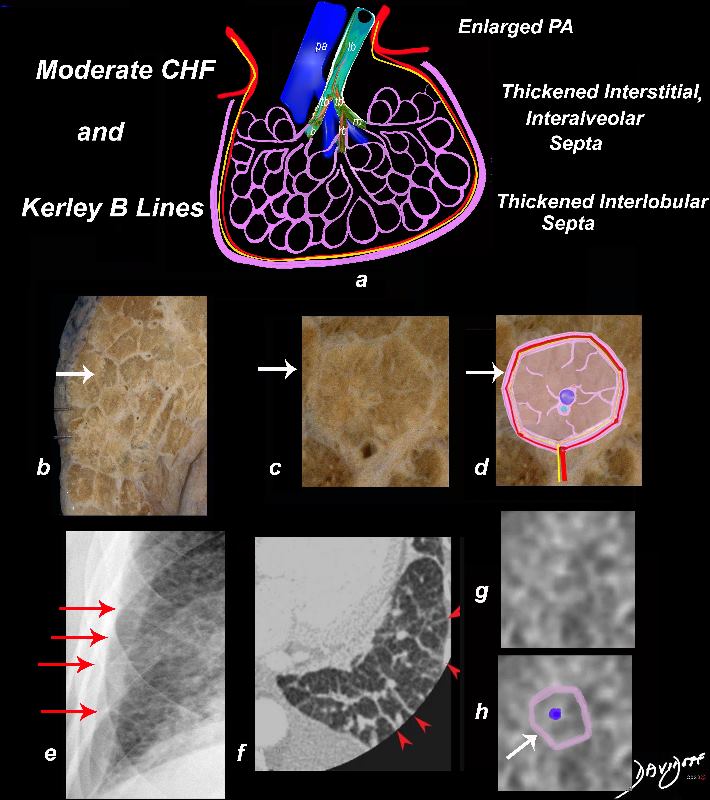
In moderate CHF, when the intravascular pressure is between 30 and 40 mmHg, it exceeds the intravascular oncotic pressure, and fluid starts to leak out of the capillaries into the interstitium. There is distension of the pulmonary arterioles, the lymphatics and thus into the interlobular septa.
The thickening of the interlobular septa (white arrows a,b,c, and d) result in the appearance of Kerley B lines on CXR (red arrows e, and red arrowheads f) . The overall increase in density caused by the fluid accumulations in the inter, and intralobular septa may result in ground glass opacity seen on the CT in images g and h.
Ashley Davidoff MD TheCommonVein.net lungs-0738 chf01b
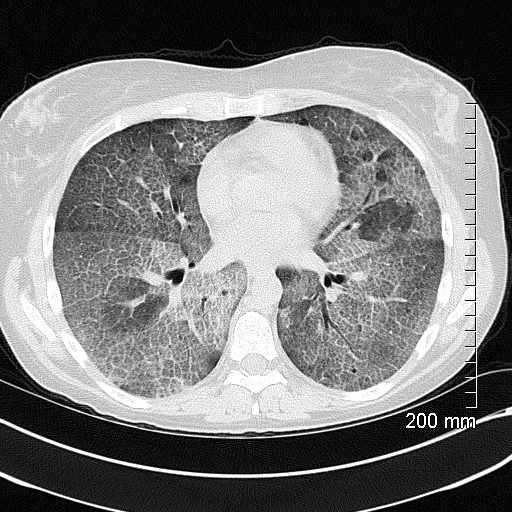
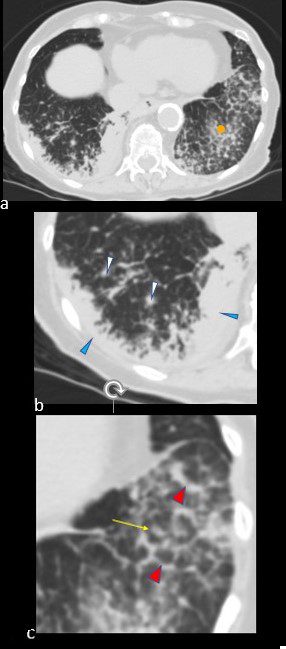
50-year-old female with diabetes, chronic renal failure and congestive heart failure. CT in the axial plane through the right posterior recess, shows thickened interlobular septa at the right base, congested arterioles (light blue arrowheads, b), alongside the bronchioles, peribronchial cuffing (white arrowheads, b), a congested pulmonary venule in the interlobular septum (red arrowhead arrowheads, b), ground glass changes and a secondary lobule demonstrating mosaic attenuation (black arrowhead arrowheads, b). The IVC is dilated and a small complex effusion is present.
Ashley Davidoff MD TheCommonvein.net 135783cL 193Lu
Thickened Interlobular Septa
Classically CHF
Lymphatics and Venules
Also reviewed in Acute Eosinophillc Pneumonia
Lymphatics
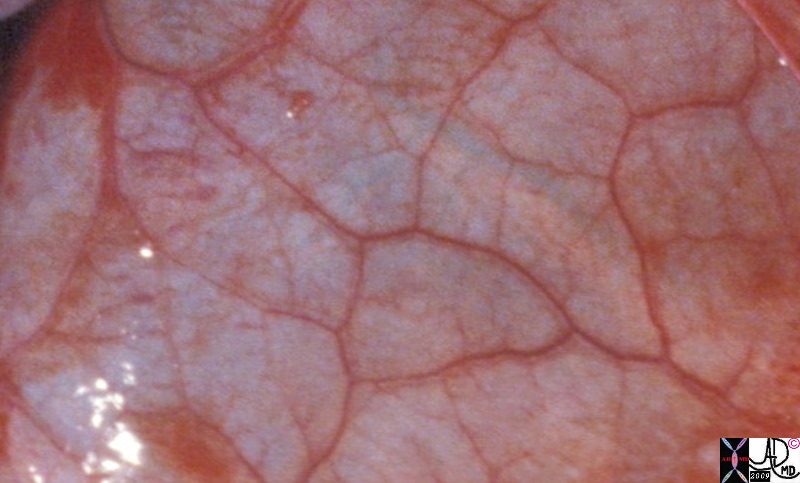
Anthracotic Lung

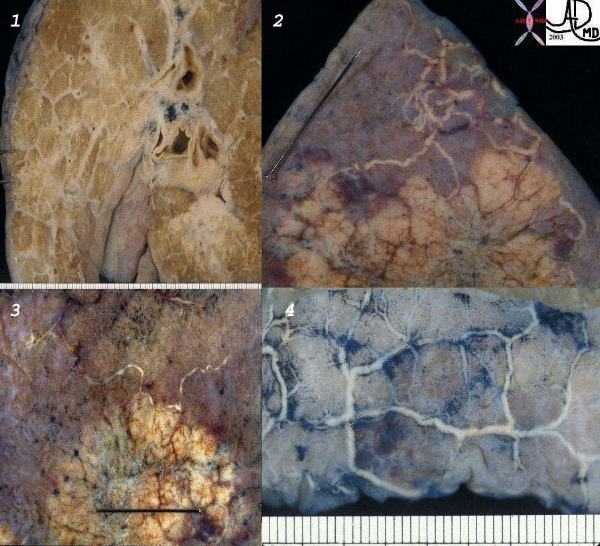
Anthracosis – Note the accumulation of carbon particles within the lymphatics along the interlobular septa, outlining the secondary lobules. The carbon particles are inhaled from an anthracotic urban environment. Courtesy Ashley Davidoff MD. 32291 code lung interlobular septum septa secondary lobule pulmonary lobule intertstitium interstitial grosspathology carbon
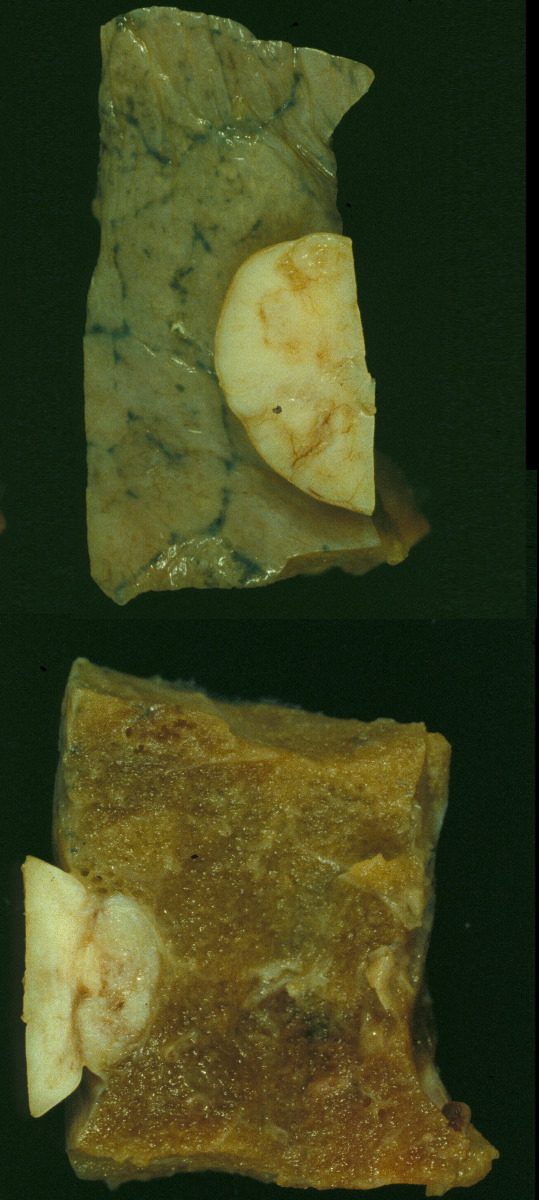
This is a post mortem specimen of a lung in a patient who had primary lung carcinoma with metastatic disease, in whom an incidental benign fibrous mesothelioma was found. The upper image reflects the external surface and the lower image the internal aspect of the lung. Note in the extrinsic mass effect on the lung in both images. Also note the accumulation of carbon in the interlobular septa in the upper image 32198c
Keywords:
lungs pulmonary pleura nodule neoplasm benign fibrous mesothelioma gross pathology
Ashley Davidoff MD TheCommonvein.net 32198c
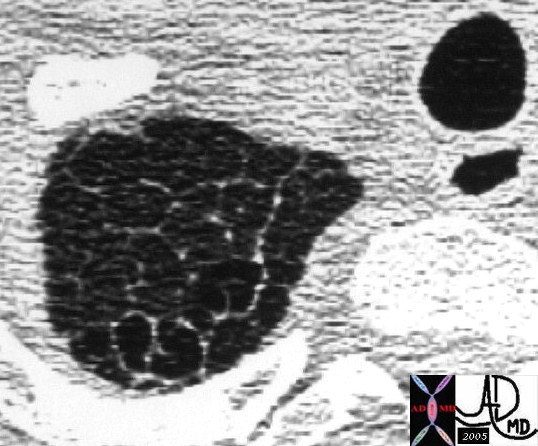
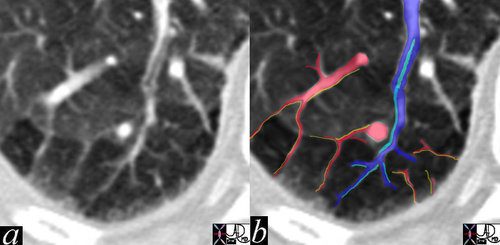
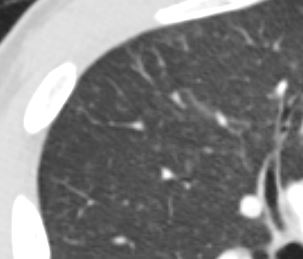
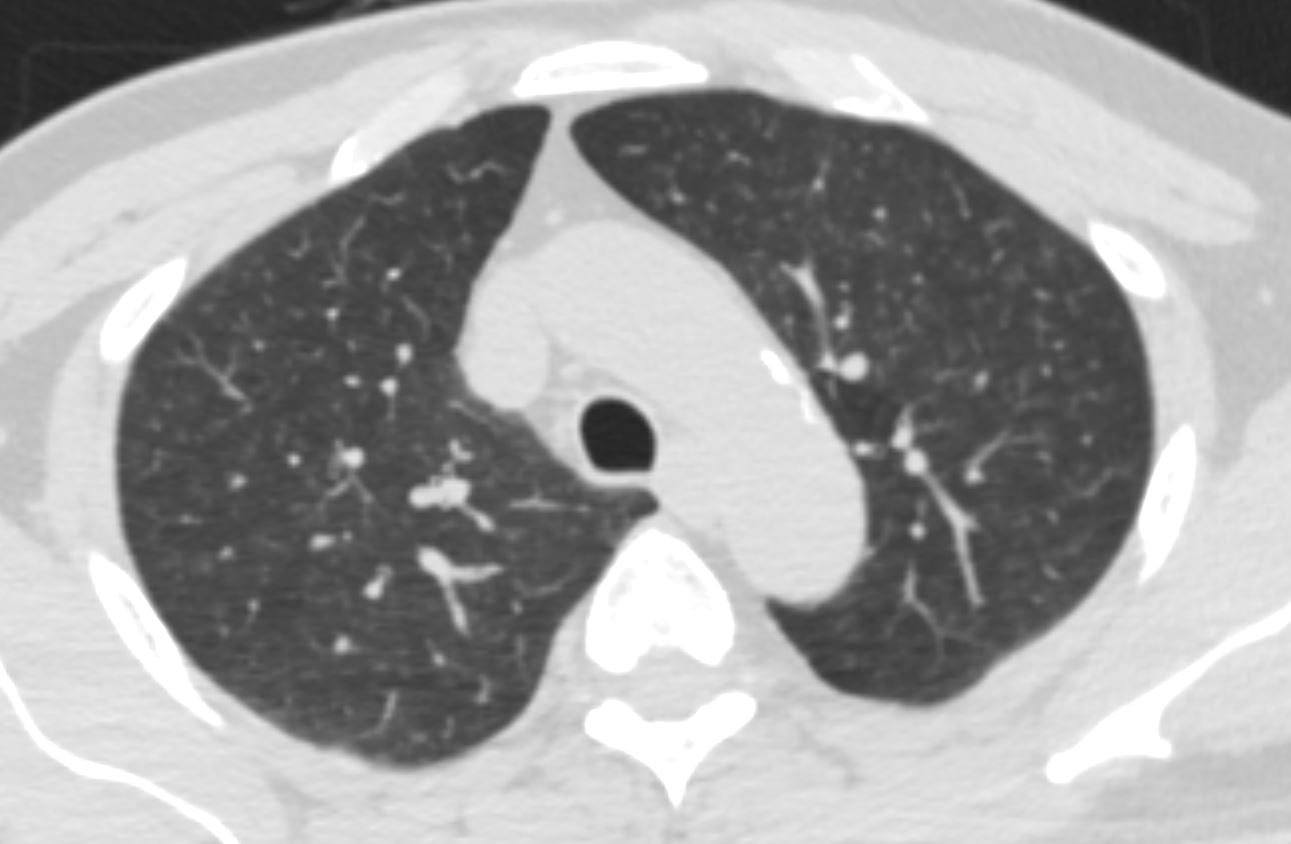
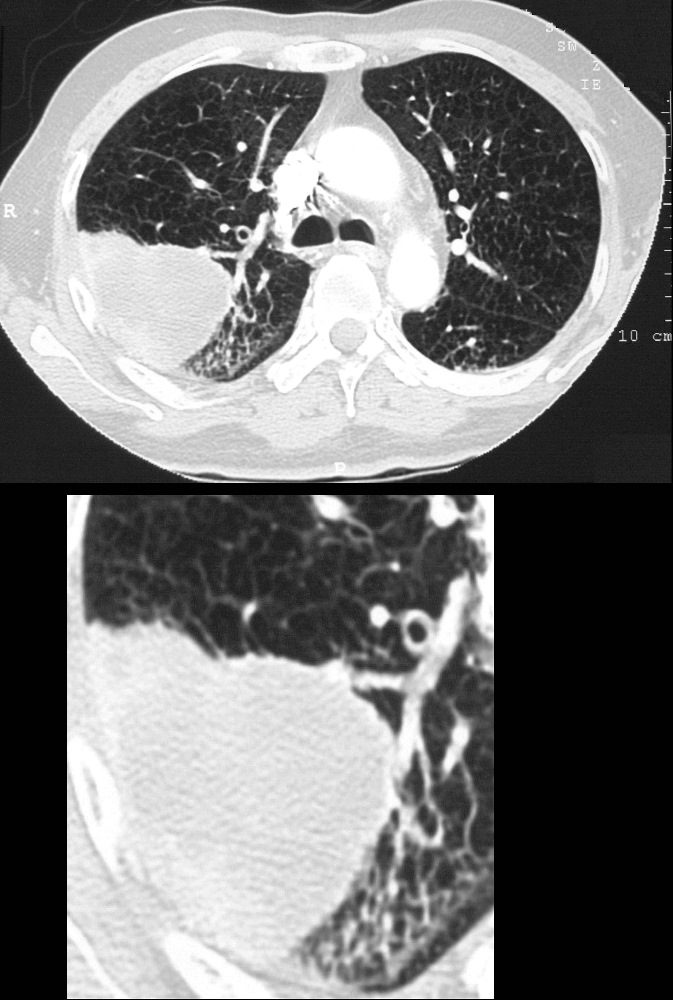
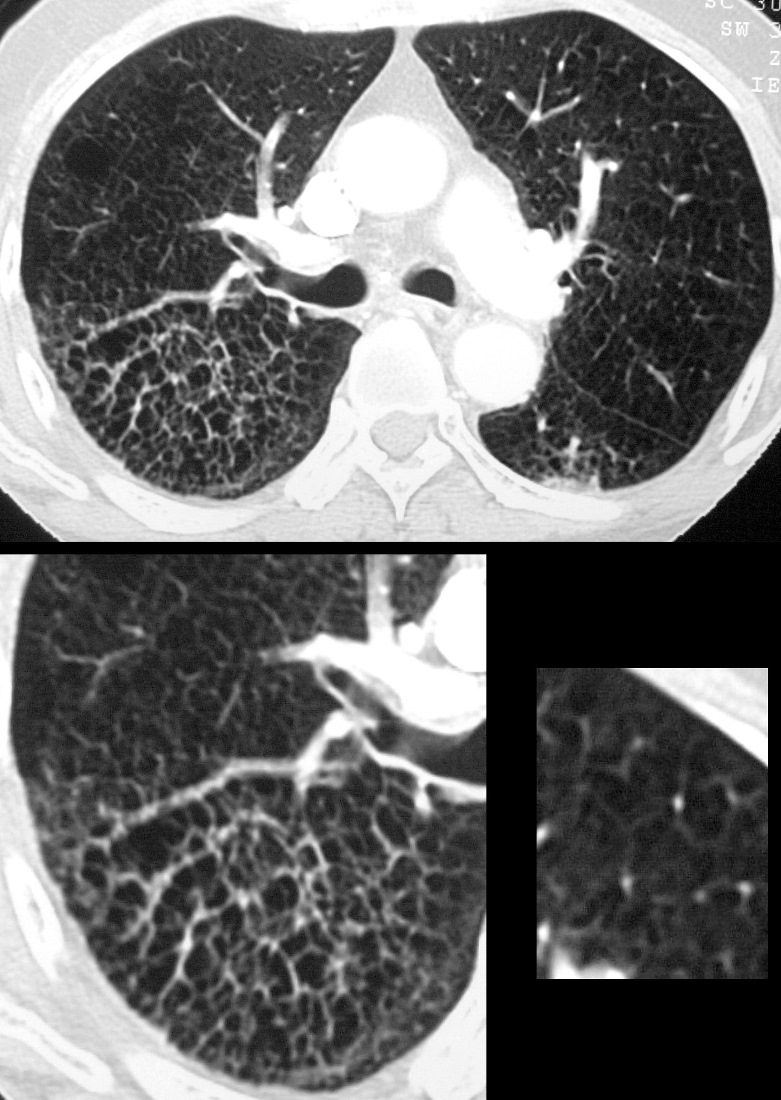
In this high resolution CTscan at the apex of the left lung the secondary lobule is seen with 3 sets of bronchovascular bundles at the door of the secondary lobule surrounded by the pulmonary venules and lymphatics in the surrounding septum. Note also that lymphatics are found both in the periphery of the lobule as well as in the centre of the lobule. This patient had mild emphysema and it was surprising to find this beautiful example of a pulmonary lobule in a patient who was almost normal. We suspect that with the higher resolution technology we will see the normal (or almost normal) pulmonary lobule with greater frequency.
Ashley Davidoff MD
TheCommonVein.net 31819
Alveolar Proteinosis
Thickened Interlobular Septa ground Glass with Crazy Paving Sign
Excellent example of crazy paving
Ashley Davidoff TheCommonVein.net 117625
CT scan through the 4 chambers of the heart using lung windows is from a a 54 year old female with SLE. Recent CXR showed bibasilar ground glass infiltrates.
The scan shows basilar multicentric infiltrates with elements of ground glass change and small airway wall thickening (red circles in the right lower lobe middle lobe and lingula, as well as interlobular septal thickening (green circle) in the lateral basal segment of the left lower lobe. A small pericardial effusion is present (yellow arrowhead)
Ashley Davidoff MD
key words SLE acute pneumonitis pericardial effusion
Lymphatic Congestion
Lymphangitis Carcinomatosis
Gross pathology specimen in the coronal plane of the right lung shows extensive irregular thickening of the interlobular septa secondary to lung cancer and lymphangitis carcinomatosis
Ashley Davidoff MD TheCommonVein.net 32327.8
TheCommonVein.net
32315c keywords
lungs pulmonary pleura secondary lobules interlobular septa thickened parenchymal nodules neoplasm lymphatics distended metastases lymphangitis obliterans gross pathology
Ashley Davidoff MD
TheCommonVein.net
32199cw
keywords
lungs pulmonary parenchymal mass neoplasm primary lymphatics distended metastases lymphangitis gross pathology
Ashley Davidoff MD
TheCommonVein.net
32226c1
keywords
lungs pulmonary neoplasm primary prostate lymphatics distended metastases lymphangitis histopathology
67-year-old man with prior history of bladder cancer. CT scan in the axial plane shows a large right upper lobe lung mass. Posterior to the mass, the interlobular septa are thickened.. These findings suggest lymphangitis carcinomatosis. Peribronchial thickening of the apical segmental airway may be due either to lymphangitis or chronic bronchitis There is background evidence of centrilobular emphysema, dominant in both upper lobes giving an internal comparison of the normal vs abnormal size of the interlobular septa
Ashley Davidoff MD TheCommonVein.net 32285c 243Lu
67-year-old man with prior history of bladder cancer. CT scan in the axial plane inferior to the lung mass shows extensive irregular thickening of the interlobular septa magnified in the right lower panel. These findings reflect lymphangitis carcinomatosis. There is background evidence of centrilobular emphysema, dominant in both upper lobes. A magnified view in the right lower panel offers an internal comparison of the abnormal vs the normal size and shape of the interlobular septa
Ashley Davidoff MD TheCommonVein.net 32287c 243Lu
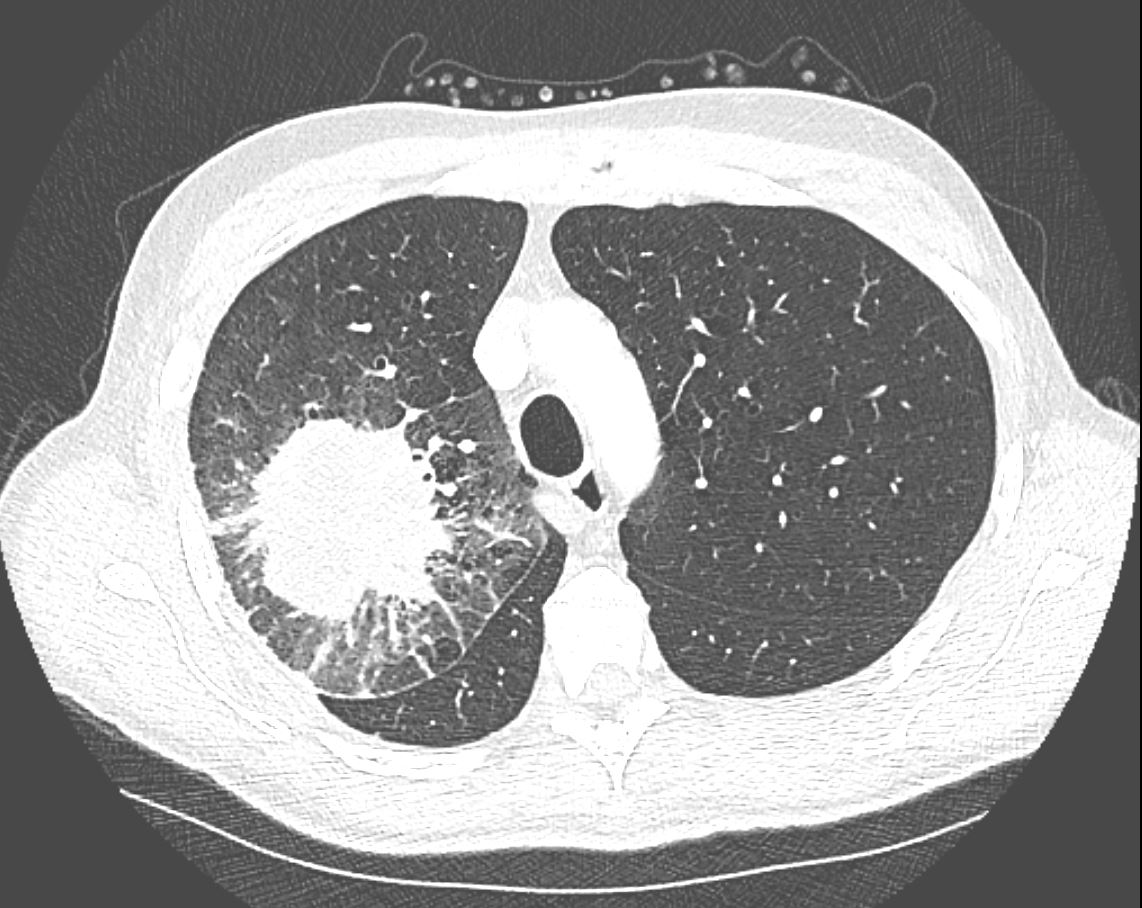
CT in the axial plane demonstrates a large, spiculated mass in the right upper lobe with surrounding halo likely reflecting hemorrhage or lymphatic edema around the mass. In addition, there is evidence of irregular interlobular septal thickening likely reflecting lymphatic invasion and indicating lymphangitis carcinomatosa. There is irregular thickening of the major fissure suggesting involvement.
Ashley Davidoff MD TheCommonVein.net 135865
Diffuse Alveolar Septal Amyloidosis
CT scan in the axial projection at the base of the lungs show many features of amyloidosis including lung nodules (white arrowheads) and infiltrates (b), and diffuse deposition within the alveolar septa (red arrowheads, c) and centrilobular nodules(yellow arrow c)
Ashley Davidoff MD Boston Medical Center
TheCommonVein.net septal-amyloidosis-001b
A Love Story

This image shows the arteriole (royal blue) and the bronchiole (teal) travelling side by side bith of equal size. Ashley Davidoff MD TheCommonVein.net 42440b05
Ashley Davidoff MD TheCommonVein.net

Here is a picture of the outside of the polyhedral pulmonary lobule from the side. It looked quite futuristic. Through the transparent side window we saw a couple similar to ourselves. From this vantage point the morphing did not look too different from what we had already been through – division after division – leaner and meaner. Ashley Davidoff MD. The Common Vein.net 42449b02
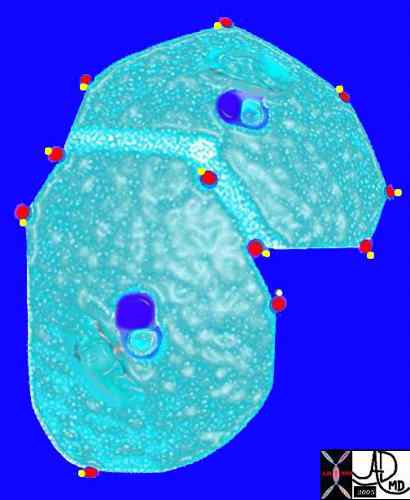
The arteriole and bronchiole lie in the center of the lobule.
Pulmonary venules (red) and lymphatics (yellow). lie in the periphery of the lobule
42440b03
Davidoff Art Courtesy Ashley Davidoff MD
This picture shows us on the left with a white ring around us (we were the tallest) and the other couples who looked so much like us (also ringed). We called our tribe the “bronchovascular bundle” with the one part of the bundle being the progeny of the bronchus and the other the progeny of the pulmonary artery. In the distance at the periphery we could see the pairs from the other friendly tribe – the red pulmonary vein with its smaller yellow buddy the lymphatic. Behind them we could see the transparent window membrane through which we had peaked earlier. Oh my goodness!!! Look what has happened to my body!!!!!!!…… Ashley Davidoff MD. The Common Vein.net 42447b03b01
This picture was taken just before the real drama started. The image gives a sense of what was to come. You can see here in the house of the lobule that we were all dividing into smaller parts and were getting smaller and the picture was quite colorful and rosy. I fully expected to have intimate contact with the arteriole… but it did not happen as I expected…… Ashley Davidoff MD. The Common Vein.net 42447b05b02
- Bronchiolar Inflammation
- AEIOU
- A
- Asthma ABPA Asbestosis
- E
- Eosinophilic Pneumonia
- Infections
- Endobronchial
- TB
- Mycobacterium
- Non TB Mycobacteria and
- Other Granulomatous Infections
- ABPA
- TB
- viruses such as
- adenovirus,
- influenza, and
- respiratory syncytial virus (RSV),
- Endobronchial
- Inflammatory
-
- Sarcoidosis
- Inhalational
- Cigarette Smoke
- smokers bronchiolitis
- Langerhans Cell
- chemicals,
- fumes, or toxic gases
- occupational exposures,
- industrial chemicals
- diacetyl in the popcorn industry
- industrial chemicals
- Cigarette Smoke
-
- Immune
-
-
- HP
- RA
- Follicular Bronchiolitis (MALT Lymphoid Hyperplasia in collagen vasc and immune deficiency)
- Graft vs Host
-
-
- Inherited
- Cystic Fibrosis
- Idiopathic Bronchiolitis Obliterans
- A
- AEIOU
- Bronchiole
-
- Endobronchial TB
- Non TB Mycobacteria and other Granulomatous Infections
- Infectious Bronchiolitis
- Cystic Fibrosis
-
- Angiocentric Disease
- CHF
- Pulmonary Hypertension
- Vasculitis
- Talicosis
- Hemorrhage
- Hemosiderosis
- Metastatic Calcification
- Lymphatic Disease
- Sarcoidosis
- Silicosis
- Coal Workers Pneumoconiosis
- Lymphangitic Disease
- LIP
- Panlobular Nodules
- Lobular Consolidation
- Bronchopneumonia
- OP
- Eosinophilic Pneumonia
- BAC Adenocarcinoma with Lepidic growth
- Lobular GGO
- Bronchopneumonia
- Viral Infection
- Mycoplasma
- PCP
- pulmonary Edema
- HP
- Alveolar Proteinosis
- Lipoid Pneumonia
- Lobular Low Attenuation
- Mosaic Attenuation
- Head Cheese Sign
- HP
- DIP
- respiratory bronchiolitis ILD
- Sarcoidosis
- Atypical Infections
- Lobular Consolidation
-
Links and References
- TCV
TCV Clinical Cases
003 Non Compaction Heart Failure and Pacemaker
Links and References
- Webb R Thin-Section CT of the Secondary Pulmonary Lobule: Anatomy and the Image—The 2004 Fleischner Lecture RadiologyVol. 239, No. 2
-

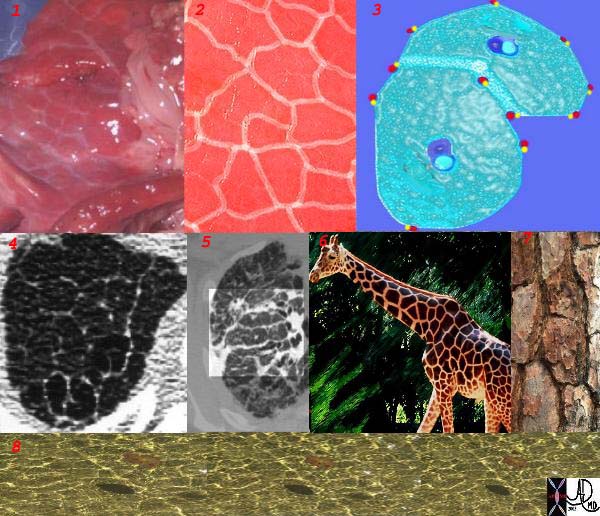
The polygonal shape of the secondary lobule can be seen all around you when you start looking
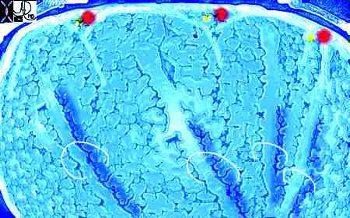
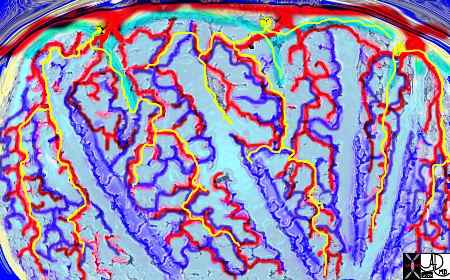
This is a series of images demonstrating the shape of the secondary lobule. The first image (1) is a post mortem specimen with congested lungs showing the interlobular septa, while the next (2), is an overlay of the septa in white showing their polygonal shape. The next drawing reveals side-by-side secondary lobules with central bronchovascular bundles and peripheral lympho-vascular bundles. Image 4 is a CT image through the apex of the lung showing thickened secondary lobules in a patient with mild emphysema, and 5 shows marked thickening of the interlobular septa in a patient with end stage sarcoidosis. 6,7,8 show the shape of the secondary lobules in the skin of a giraffe, the bark of a pine, and the ripples of the water respectively.
Ashley Davidoff MD TheCommonVein.net 31866collage