
Etymology
- The term “silhouette” originates from the French name “Etienne de Silhouette,” a French finance minister known for his minimalist portraits. In radiology, it refers to the loss of visible borders between two structures of similar density.
AKA
- None.
What is it?
- The silhouette sign is a radiologic finding characterized by the loss of the normal outline or border of adjacent thoracic structures due to the presence of a lesion or pathology with similar radiographic density.
- It is most commonly observed on chest X-ray (CXR) and helps localize a pathology within the thorax.
Characterized by
- Loss of a well-defined border between:
- Lung and heart,
- Lung and diaphragm, or
- Lung and chest wall.
- It indicates that a pathological process (e.g., fluid, mass, or consolidation) of soft-tissue density is in direct contact with the structure, obscuring its border.
Anatomically affecting
- The sign can occur in various thoracic regions based on the affected anatomical structures:
- Right heart border → Middle lobe pathology.
- Left heart border → Lingula of the left upper lobe.
- Right hemidiaphragm → Right lower lobe pathology.
- Left hemidiaphragm → Left lower lobe pathology.
- Aortic arch → Left upper lobe pathology.
- Descending aorta → Left lower lobe or posterior mediastinum pathology.
- Right paratracheal region → Right upper lobe pathology.
Causes include
- Most Common Causes:
- Consolidation (e.g., lobar pneumonia).
- Other Causes include:
- Infection:
- Bacterial pneumonia (e.g., Streptococcus pneumoniae).
- Fungal infections (e.g., histoplasmosis, aspergillosis).
- Neoplasm:
- Lung cancer (e.g., bronchogenic carcinoma).
- Mediastinal masses (e.g., lymphoma).
- Inflammation:
- Atelectasis with collapse of lung segments.
- Pulmonary edema.
- Fluid:
- Pleural effusion (adjacent to diaphragm or chest wall).
- Other Pathologies:
- Chest wall lesions or mediastinal abnormalities.
- Infection:
Pathophysiology
- Normally, adjacent thoracic structures (e.g., lung, heart, diaphragm) are distinguishable on imaging due to differences in radiographic density.
- The silhouette sign occurs when a pathological process (e.g., consolidation, mass, fluid, or atelectasis) eliminates the normal density contrast between two adjacent structures, making the border indistinct.
Histopathology
- Pathology depends on the underlying cause:
- Consolidation: Alveolar spaces filled with inflammatory exudate.
- Neoplasm: Tumor cells replacing normal lung tissue.
- Pulmonary edema: Accumulation of fluid in alveolar spaces.
Imaging
Applied Anatomy
- Parts: Adjacent thoracic structures such as the heart, diaphragm, and mediastinum.
- Size: Varies depending on the size of the pathological lesion.
- Shape: Indistinct or blurred margins of normally well-defined structures.
- Position: Based on the anatomical region in contact with the pathology.
- Character: Uniform soft tissue density which can be due to alveoli filled with fluid, blood, pus, inflammatory cells or tumor cells, or due to atelectasis, obscuring an adjacent border.
- Time: Can be acute (e.g., pneumonia) or chronic (e.g., mass or fibrosis).
CXR
- Key Modality for Detection:
- Loss of the normal border or silhouette of thoracic structures.
- Examples:
- Right heart border obscured → Middle lobe consolidation.
- Left heart border obscured → Lingula consolidation.
- Right hemidiaphragm obscured → Right lower lobe consolidation.
- Left hemidiaphragm obscured → Left lower lobe consolidation.
- Aortic arch silhouette obscured → Left upper lobe pathology.
- Associated findings:
- Air bronchograms in consolidation.
- Adjacent pleural effusion may enhance the silhouette sign.
CT
- Confirms the CXR findings and provides detailed anatomical localization:
- Consolidation, mass, or pleural fluid adjacent to specific structures.
- Helps identify subtle pathology, particularly in complex or overlapping regions.
- Air bronchograms, mediastinal lymphadenopathy, or pleural involvement may be present.
- Examples:
- Middle lobe collapse or consolidation adjacent to the right heart border.
- Lingular pathology obscuring the left heart border.
MRI
- Limited role in evaluating the silhouette sign but can help characterize mediastinal masses.
PET-CT
- Useful in evaluating masses or malignancies obscuring normal thoracic silhouettes.
- Increased metabolic activity helps differentiate neoplastic from benign processes.
Differential Diagnosis
- Lobar pneumonia: Most common cause of the silhouette sign.
- Atelectasis: Collapse of a lung segment leading to obscured borders.
- Pleural effusion: Fluid accumulation adjacent to the diaphragm or chest wall.
- Lung masses: Tumors adjacent to thoracic structures.
- Pulmonary edema: Bilateral hazy opacities may obscure thoracic structures.
- Chest wall or mediastinal lesions: Abnormalities directly in contact with the pleura.
Recommendations
- Further Imaging:
- Chest CT for confirmation and localization of pathology.
- Contrast-enhanced CT for evaluating masses or vascular involvement.
- Laboratory Correlation:
- Blood cultures, sputum analysis for infection.
- Tumor markers in suspected malignancy.
- Functional Assessment:
- Pulmonary function tests (PFTs) if chronic pathology is suspected.
- Biopsy: For masses or unclear findings on imaging.
Key Points and Pearls
- The silhouette sign helps localize pathology within the thorax based on the obscured anatomical border.
- It most commonly indicates consolidation (e.g., lobar pneumonia).
- A clear understanding of thoracic anatomy is essential for interpreting the silhouette sign.
- CT provides more precise localization and characterization of the underlying pathology.

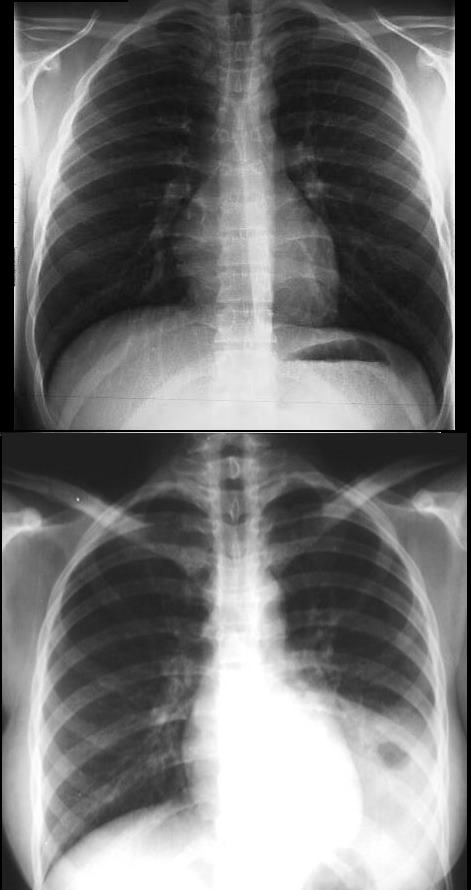
52 year old male presents with a cough and fever
Frontal CXR shows a lingular infiltrate with a positive silhouette sign. Both the superior and inferior lingular segments appear to be involved
Ashley Davidoff MD TheCommonVein.net

52 year old male presents with a cough and fever
Lateral CXR shows a dense lingular infiltrate overlying the heart. Both the superior and inferior lingular segments appear to be involved
Ashley Davidoff MD TheCommonVein.net
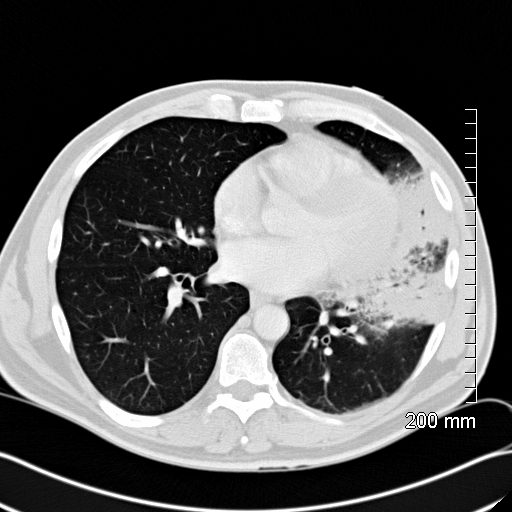
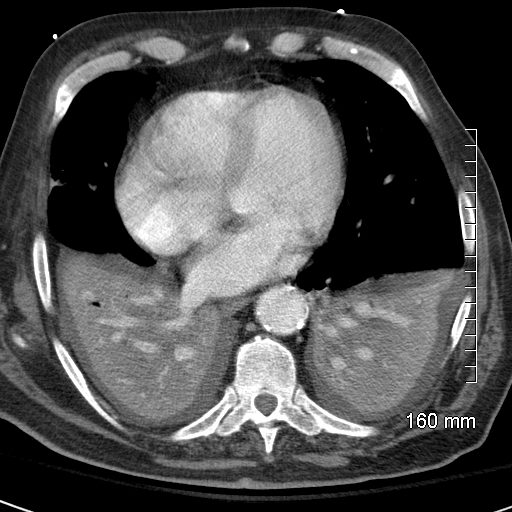
52 year old male presents with a cough and fever
CT scan in the axial plane shows a lingular consolidation with air bronchograms and a positive silhouette sign. Both the superior and inferior lingular segments are involved
Ashley Davidoff MD TheCommonVein.net
Source
Signs in Thoracic Imaging
Journal of Thoracic Imaging 21(1):76-90, March 2006.
- This classic roentgenographic sign
-
- first described by Felson in 1950
- “an intrathoracic lesion touching a border of the heart, aorta, or diaphragm will obliterate that border on the roentgenogram. An intrathoracic lesion not anatomically contiguous with a border of one of these structures will not obliterate that border.”
- The right heart border silhouette
- indicates right middle lobe process
- The left heart border silhouette
- first described by Felson in 1950
- silhouette sign
- cervicothoracic and hilum overlay sign.
-
Why We See Things
Ashley Davidoff thecommonvein.net
Ashley Davidoff thecommonvein.net
Ashley Davidoff thecommonvein.net
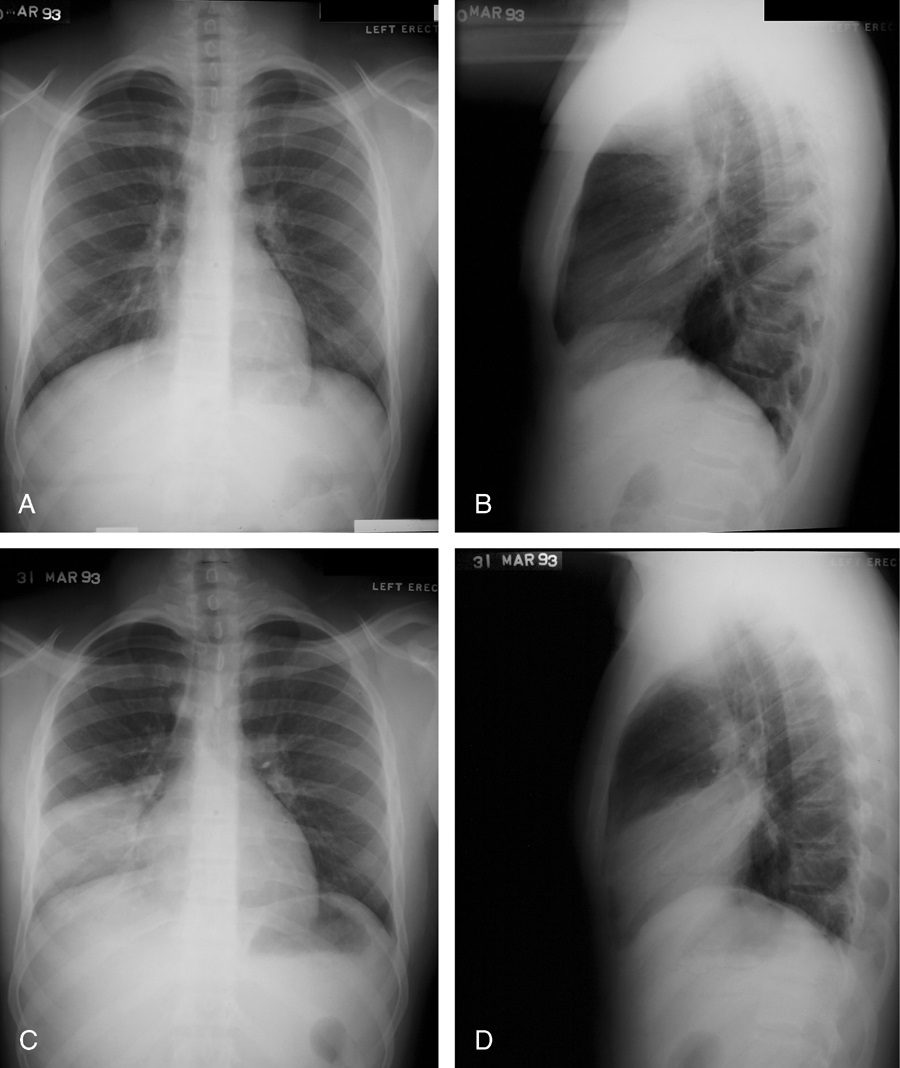
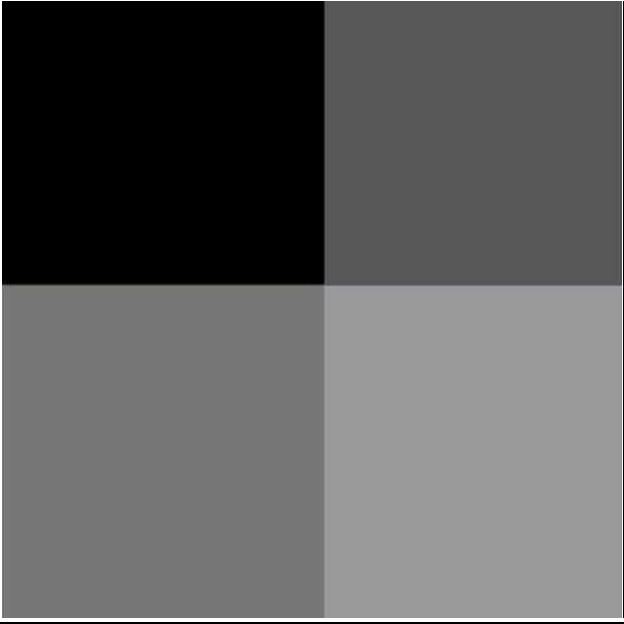
Silhouetting
In the Top Image
Why we see the left hemidiaphragm – Contrast of Black on White
Why we see the air – fluid level in the stomach – Black on White
In the Bottom image
Why we do not see the left hemidiaphragm
Because the alveoli are filled with pus from a left lower lobe pneumonia and we have white on white
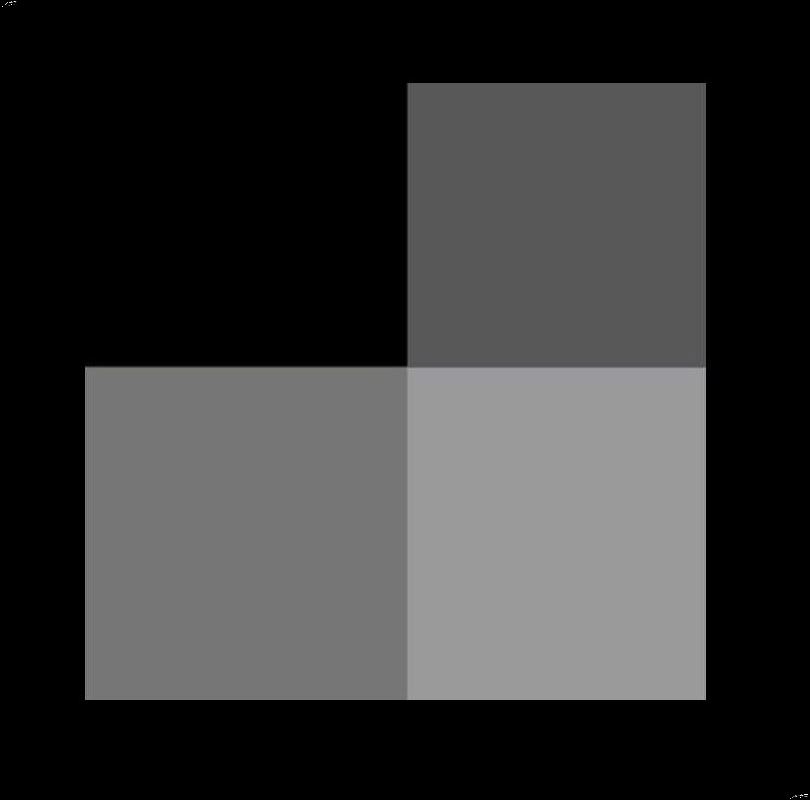
When the alveoli are filled with air the thin walled smaller airways are not visualized (equivalent of silhouetted) However when they become filled with fluid eg pus blood malignant cells the contrast between the air and fluid or soft tissue created the air bronchogramWhen the Alveoli are Filled with Fluid

When the alveoli are fully filled with fluid, tumor, or pus for example, the overall net density will be white, and when adjacent to air filled airways, air bronchograms are visible (left side of image)
When the alveoli are only partially filled, the density of the fluid added to the density of the air results in an overall gray density, and when positioned next to air filled bronchi, there is insufficient contrast to create an air bronchogram and sufficient to enable visualization of the blood vessels. This is called ground glass opacification
Ashley Davidoff
TheCommonVein.net lungs-00681
On the Other Hand….
When there is consolidation and we do not see the silhouette sign it implies the airways are filled with a soft tissue density – like in aspiration pneumonia
74 year old male alcoholic with bilateral basilar lobar atelectasis caused by bilateral aspiration
CT scan shows airless lower lobes with small bilateral effusions.
Ashley Davidoff MD TheCommonVein.net RnD image 236Lu
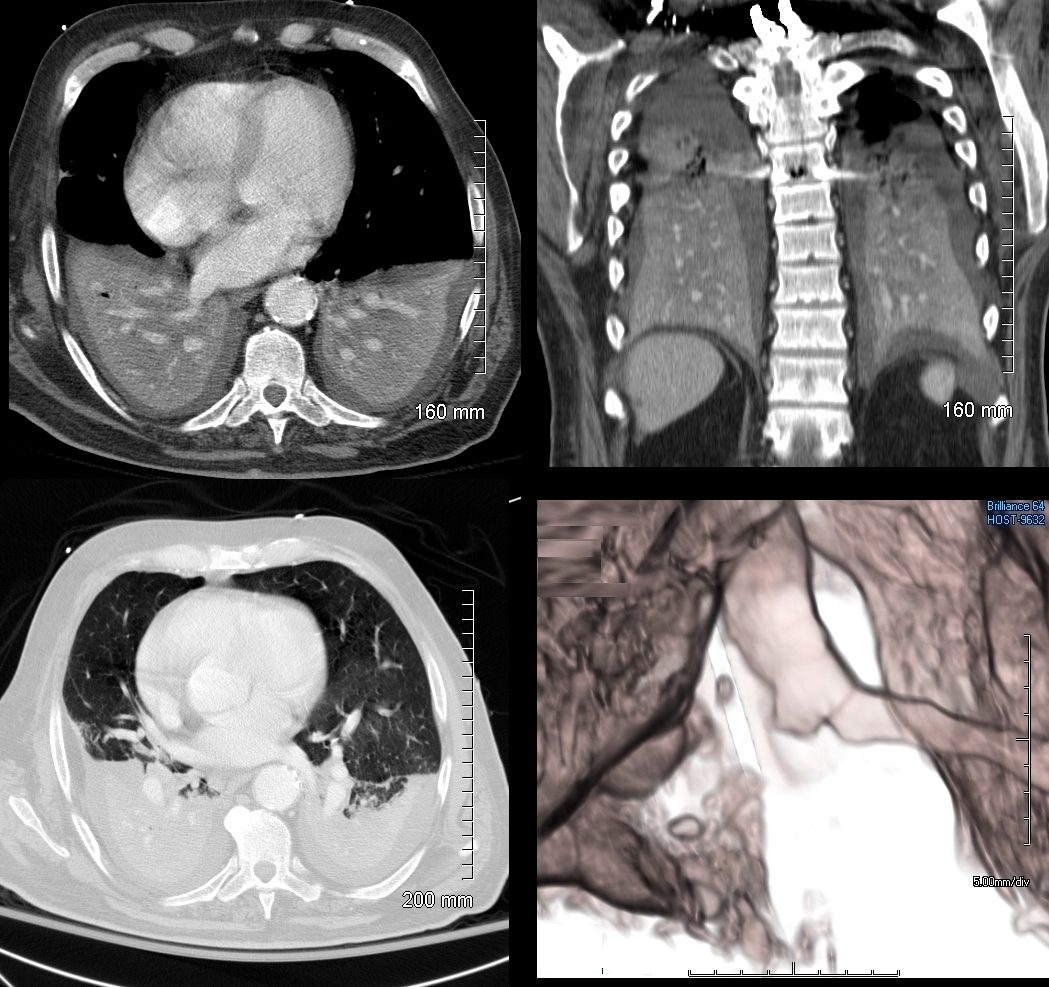
74 year old male alcoholic with bilateral basilar lobar atelectasis caused by bilateral aspiration
CT scan shows airless lower lobes with small bilateral effusions. 3D reconstruction shows total obstruction of the right mainstem bronchus, and patent proximal mainstem bronchus
Ashley Davidoff MD TheCommonVein.net 236Lu
Parallels with Human Endeavors
The silhouette sign highlights the concept of contrast and visibility, which has applications across art, design, and nature:
- Art: Silhouettes in painting and photography rely on contrast to define edges and forms.
-

Sainte Madeleine and Sainte Catherine,” ca. 1440. Konrad Witz,
A Shadow on Saint Madeline’s Green Dress prevents us from appreciating the detailed folds
Strasbourg, Musée de l’Oeuvre Notre-Dame.Der Sterbende, Epitaph des Heinrich Schmitburg 1518
Note the loss of detail of the shoes of the man in red robes and the differential diagnosis would be for example a consolidation, whereas the shadow on the shoes of the man in green clothes is not as dark, and the density can be equated to a ground glass density Lucas Cranach the Elder (1472–1553)
Museum der bildenden Künste. Image credit: Cranach Digital Archive. - Architecture: Shadow patterns used to obscure or highlight features in buildings.
-
Using Shadows in Architecture
Zeitz Museum of Contemporary Art Africa
Courtesy Christo Goosen - Literature: Hidden or obscured themes that only become visible through careful analysis.
- Quotes
- “Light and shadow are opposite sides of the same coin. We can illuminate our paths or darken our way. It is a matter of choice.”
– Maya Angelou - “All the darkness in the world cannot extinguish the light of a single candle.”
– St. Francis of Assisi - “Sometimes our light goes out, but is blown again into instant flame by an encounter with another human being.”
– Albert Schweitzer
- “Light and shadow are opposite sides of the same coin. We can illuminate our paths or darken our way. It is a matter of choice.”
- Nature: Camouflage in animals, where similar coloration blends structures with their background.
-
Lizard Camouflaged Against the Bark of a Tree tree
Similar coloe and Density Results in the Equivalent of Shadowing on a CXR
Courtesy Mikkel Houmøller - Design: Use of negative space to create visual emphasis in logos and illustrations.
Edith Farnsworth House by Mies van der Rohe
Stark Enabling Emphasis and Contrast reflecting the oppposite regarding shadowing nd silhouetting in Radiology
Victor Grigas/Wikimedia Commons [





This radiologic sign underscores how loss of contrast—whether in art, nature, or imaging—can obscure essential details, requiring deeper investigation for clarity and understanding.