
- Etymology
The term “tree-in-bud” is derived from its resemblance to budding trees, symbolizing the growth and renewal of spring. - AKA
None. - What is it?
- A radiological finding characterized by:
- Branching linear opacities resembling a budding tree, and
- Small centrilobular nodules representing impacted or dilated small airways.
- Typically indicates endobronchiolar inflammation or obstruction, often seen in infectious and inflammatory processes.
- A radiological finding characterized by:
- Characterized by
- Involvement of:
- Bronchioles,
- Alveolar ducts, and
- Small airways within the centrilobular region.
- Reflects distal airway disease with intraluminal filling by mucus, pus, or fluid.
- Involvement of:
- Anatomically affecting
- Terminal bronchioles, extending to the alveolar ducts.
- Centrally distributed within the secondary pulmonary lobule, often in the lower lobes or peripheral lung zones.
- Causes include
- Most Common Causes
- Infection:
- Tuberculosis (including post-primary/endobronchial TB).
- Mycobacterium avium complex (MAC).
- Infection:
- Other Causes include
- Infection:
- Viral: Respiratory syncytial virus (RSV), measles.
- Fungal: Aspergillosis, bronchocentric histoplasmosis.
- Inflammation:
- Bronchiolitis (including respiratory and follicular types).
- Immune:
- Allergic bronchopulmonary aspergillosis (ABPA).
- Aspiration:
- Recurrent inhalation of gastric contents or foreign materials.
- Infection:
- Most Common Causes
- Pathophysiology
- Distal airway obstruction and inflammation lead to dilation of bronchioles.
- Intraluminal filling by inflammatory cells, mucus, or pathogens causes the tree-in-bud appearance.
- Histopathology
- Histological findings include:
- Lymphocytic infiltration and peribronchiolar inflammation.
- Intraluminal debris, such as mucus, pus, or infectious material.
- Histological findings include:
- Imaging Radiology
- Applied Anatomy to CT
- Parts: Terminal bronchioles and alveolar ducts.
- Size: Centrilobular nodules typically measure 2–3 mm.
- Shape: Branching, tree-like structures with nodular buds.
- Position: Centrilobular, predominantly in the lower lobes or peripheral lung zones.
- Character: Soft-tissue attenuation nodules and linear opacities.
- Time: Acute or chronic, depending on the etiology.
- CXR
- Rarely detects tree-in-bud findings due to their small size.
- Advanced cases may show diffuse or focal nodular opacities suggesting small airway disease.
- MRI
- Limited role in small airway disease.
- T2-weighted sequences may highlight fluid-filled airways as hyperintense signals.
- PET-CT
- Primarily used for unclear etiologies or suspected malignancy.
- Increased FDG uptake may indicate active infection or inflammation.
- Other
- Bronchography (historical): Reveals dilated bronchioles with terminal filling defects.
- Applied Anatomy to CT
- Differential Diagnosis
- Bronchiectasis: Larger airway dilation without the characteristic nodular opacities.
- Pulmonary fibrosis: Reticular patterns with architectural distortion.
- Miliary nodules: Random distribution without branching.
- Recommendations
- Perform CT imaging for detailed evaluation of small airway involvement.
- Evaluate for infections with sputum analysis, AFB staining, and cultures.
- Consider bronchoscopy for direct sampling.
- Use PET-CT if masses or neoplasms are suspected.
- Key Points and Pearls
- The tree-in-bud pattern is a hallmark of endobronchial infection, particularly tuberculosis and MAC.
- The finding is diagnostic of small airway disease and reflects distal bronchiolar involvement.
- Chronic cases suggest immune dysfunction, aspiration, or non-infectious inflammation.
The Tree-in-Bud (TIB) sign is a radiological finding observed on high-resolution CT (HRCT) of the chest. It represents centrilobular branching opacities with a nodular appearance, resembling budding tree branches. This sign typically indicates a pathological process within the small airways, such as bronchioles, and is often associated with infectious or inflammatory diseases.
Tree-in-bud is a radiological pattern seen on high-resolution CT
scans of the lungs, characterized by small, branching opacities that
resemble budding branches of a tree. This appearance is caused by
the impaction of mucus, pus, or other material within the small
airways (bronchioles), often due to infection, inflammation, or
aspiration. The pattern is commonly associated with conditions
such as bronchiectasis, tuberculosis, bacterial or viral
bronchiolitis, cystic fibrosis, and mycobacterial infections. The
pathogenesis involves the filling of the bronchioles and nearby
alveolar ducts with infectious or inflammatory material, leading to a
localized airway obstruction and subsequent peripheral opacities
on imaging. Diagnosis relies on the characteristic tree-in-bud
pattern seen on CT, along with clinical evaluation and sometimes
sputum cultures or bronchoscopy to identify the underlying cause. (Neelou)
Ashley Davidoff
TheCommonVein.net

Ashley Davidoff
TheCommonVein.net
Anatomical Basis
The Small Airways
Alveolar Ducts and Alveolar Sacs
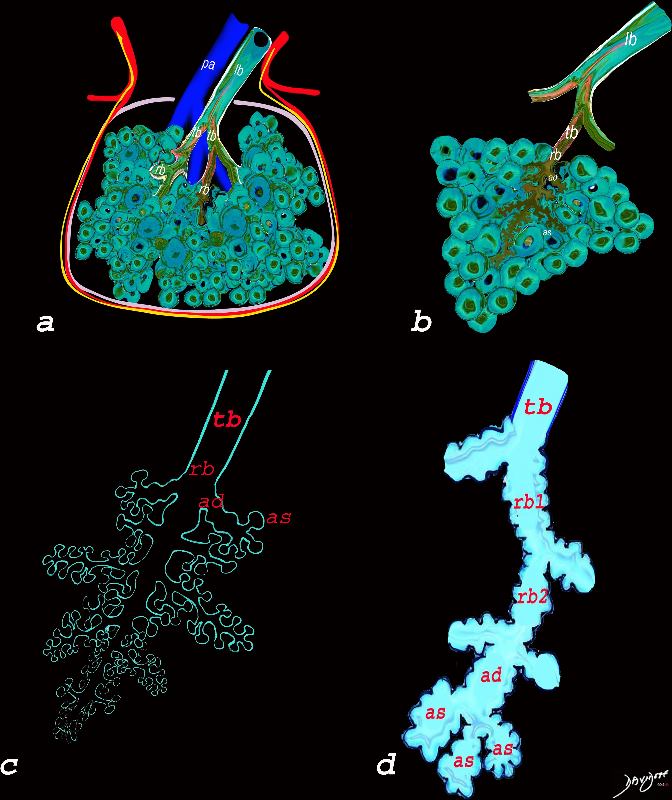
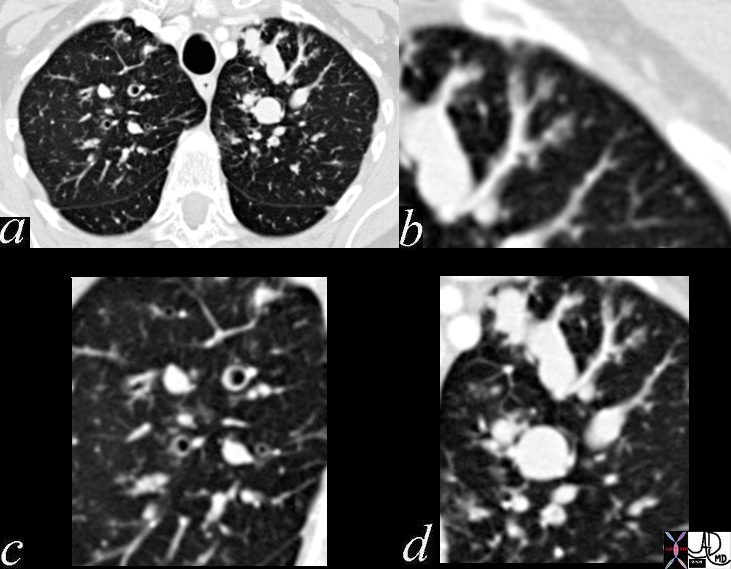
The diagram allows us to understand the the components and the position of the small airways starting in (a) which is a secondary lobule that is fed by a lobular bronchiole(lb) which enters into the secondary lobule and divides into terminal bronchioles (tb) which is the distal part of the conducting airways, and at a diameter of Ashley Davidoff MD TheCommonVein.net lungs-0744
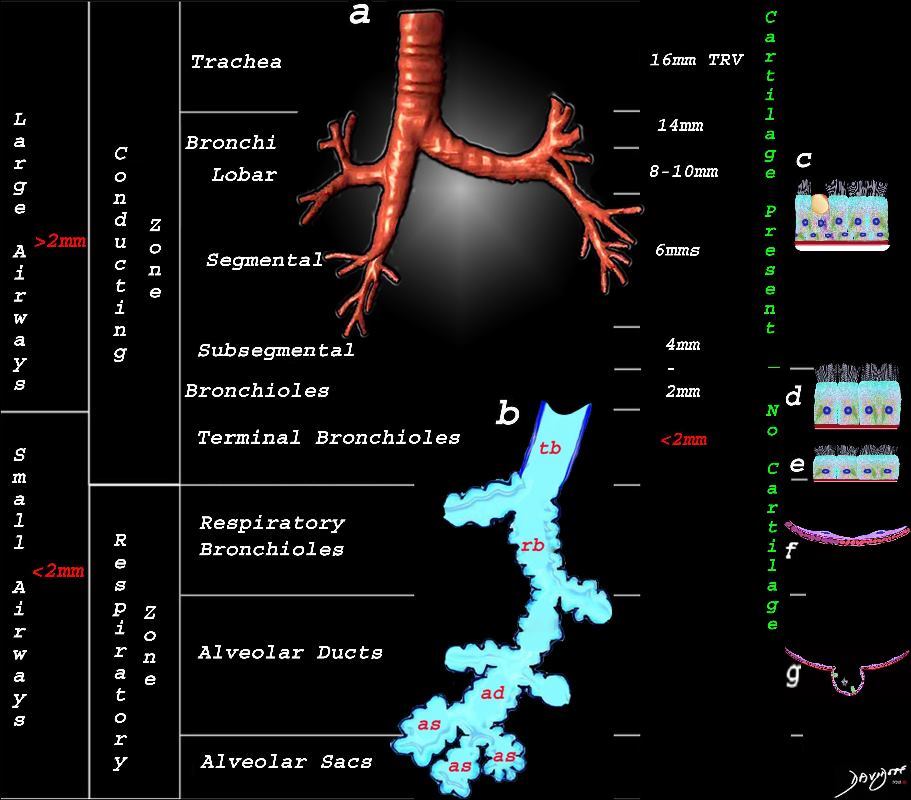
This image shows the division of the airways in the lungs classified as large airways and small airways.
A large airway is considered any airway larger than 2mm, and therefore includes all the airways involved with transport of air except for the terminal bronchiole. Included as seen in image a, are the trachea, mainstem bronchi, lobar bronchi segmental and subsegmental airways and the 3 subsequent divisions of subsegmental bronchi and bronchioles till the last transporting airway – the respiratory bronchiole which is usually about 2mm and is considered a small airway Image (a) shows the airways starting in the trachea and continuing to the mainstem bronchi, lobar bronchi, segmental bronchi, and subsegmental bronchi.
Image b shows the structures that make up the small airways starting with the terminal bronchiole (tb) followed by the respiratory bronchiole (rb) alveolar duct, (ad) and alveolar sacs (as)
Image (c) shows the histologic makeup of the large airways that include a pseudostratified ciliated columnar epithelium with mucus secreting goblet cells a muscular layer (red) and a prominent cartilage layer (white) In the larger bronchioles (d) the epithelium remains as a pseudostratified, ciliated, columnar epithelium with prominent muscular layer (red). The columnar epithelium transitions to a stratified ciliated cuboidal epithelium by the terminal bronchiole s (f) both still with a muscular layer. The respiratory epithelium transitions from a cuboidal epithelium to a squamous epithelium (f) with alveoli and type I and II pneumocytes starting to branch (g)
Ashley Davidoff MD TheCommonVein.net lungs-0740nL
Pathophysiology
The Tree-in-Bud pattern results from:
- Endobronchial spread of material:
- Mucus, pus, or other substances accumulate within the bronchioles.
- Peribronchiolar inflammation:
- Thickening of the walls of small airways and their surrounding structures.
- Distal airway obstruction:
- Often due to infection or inflammatory debris.
Radiological Features
- Appearance:
- Centrilobular, branching opacities resembling a tree with buds on its branches.
- Composed of:
- Linear structures (the “branches”): Reflect dilated or inflamed bronchioles.
- Small nodules (the “buds”): Represent impacted bronchioles or peribronchiolar inflammation.
- Location:
- Centrilobular distribution: Centered within secondary pulmonary lobules.
- Predominantly affects the lower lobes but may involve other areas depending on the underlying disease.
- Associated Findings:
- Ground-glass opacities.
- Consolidation or airspace filling in advanced stages.
Common Causes
- Infectious Causes:
- Bacterial:
- Tuberculosis (particularly in active or post-primary stages).
- Nontuberculous mycobacterial infections (e.g., Mycobacterium avium complex).
- Fungal:
- Aspergillosis.
- Viral:
- Viral pneumonias can rarely mimic this appearance.
- Parasitic:
- Parasitic infections like ascariasis or strongyloidiasis can rarely cause TIB.
- Bacterial:
- Inflammatory Conditions:
- Bronchiectasis:
- Associated with chronic airway inflammation and infections.
- Cystic Fibrosis:
- TIB is common due to recurrent infections.
- Hypersensitivity Pneumonitis:
- Inflammatory reaction causing small airway involvement.
- Bronchiectasis:
- Aspiration:
- Recurrent aspiration leading to chronic bronchiolar inflammation.
- Diffuse Panbronchiolitis:
- Seen primarily in East Asian populations, associated with chronic infection.
- Connective Tissue Diseases:
- Rheumatoid arthritis-associated bronchiolitis.
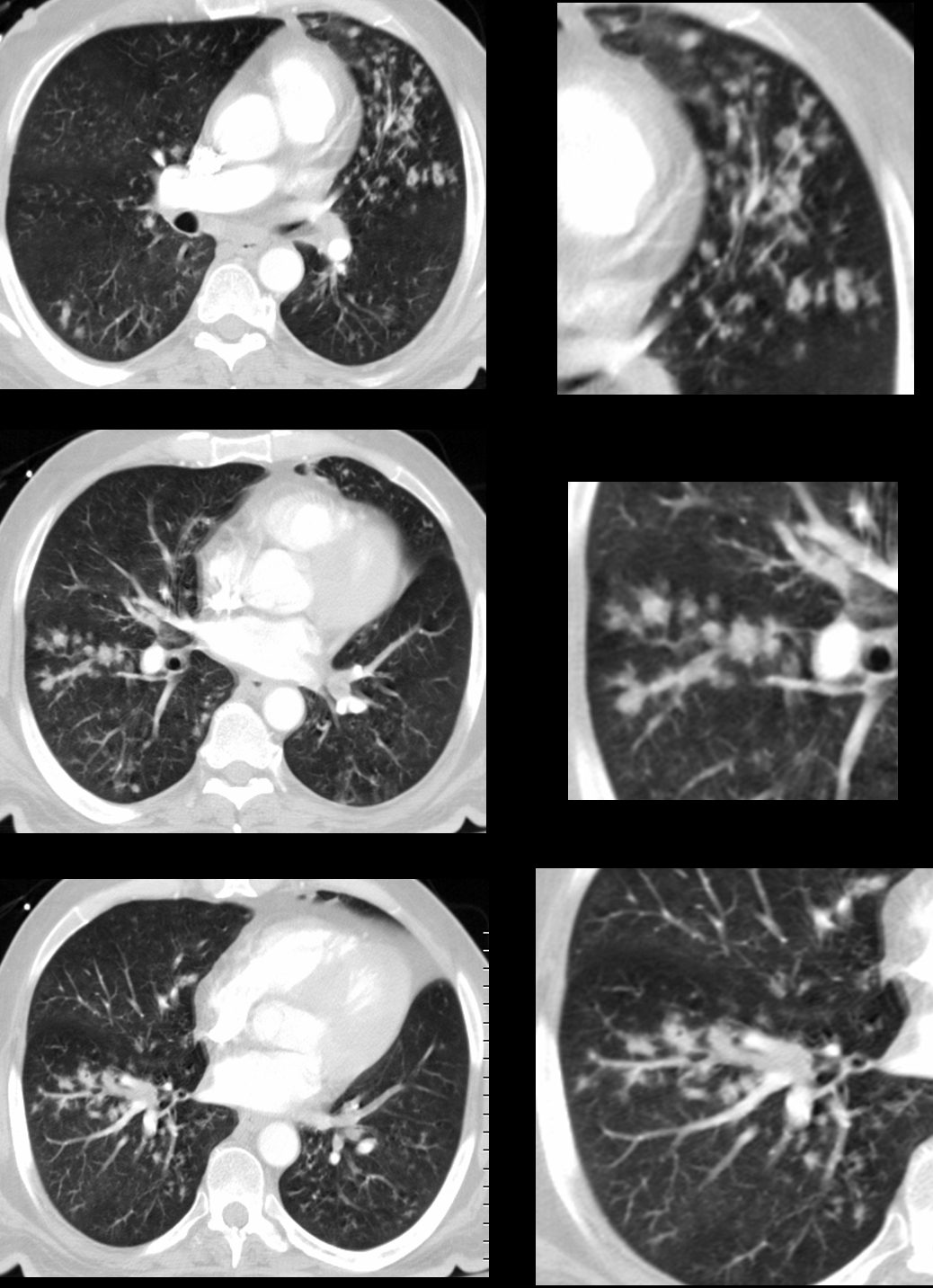
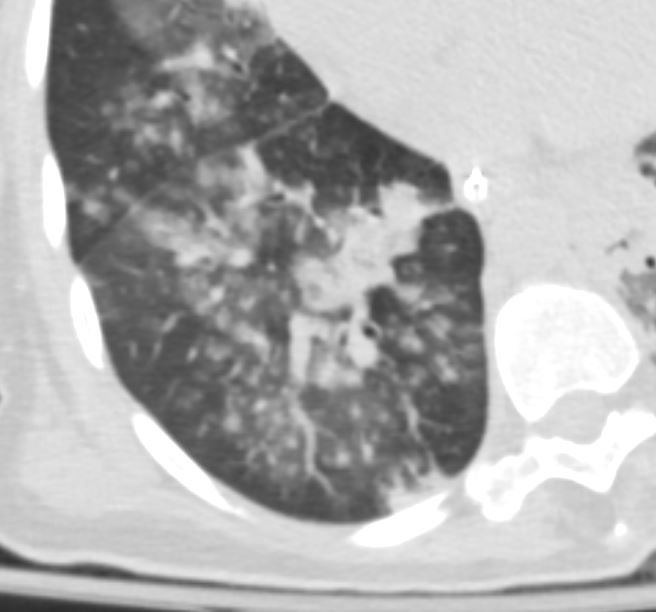
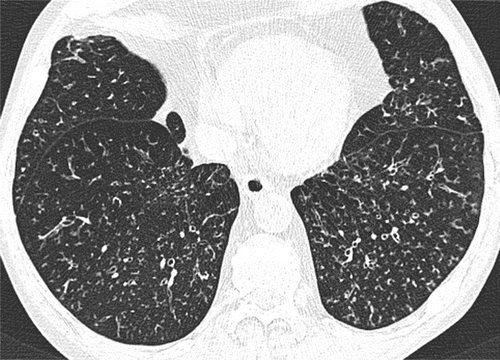
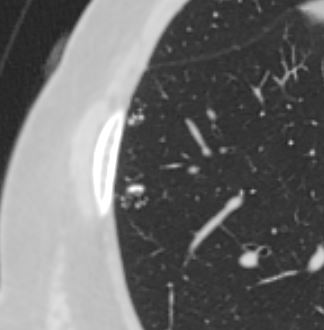
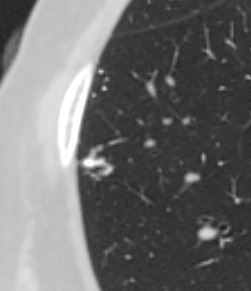
Reactivation TB with Transbronchial Spread
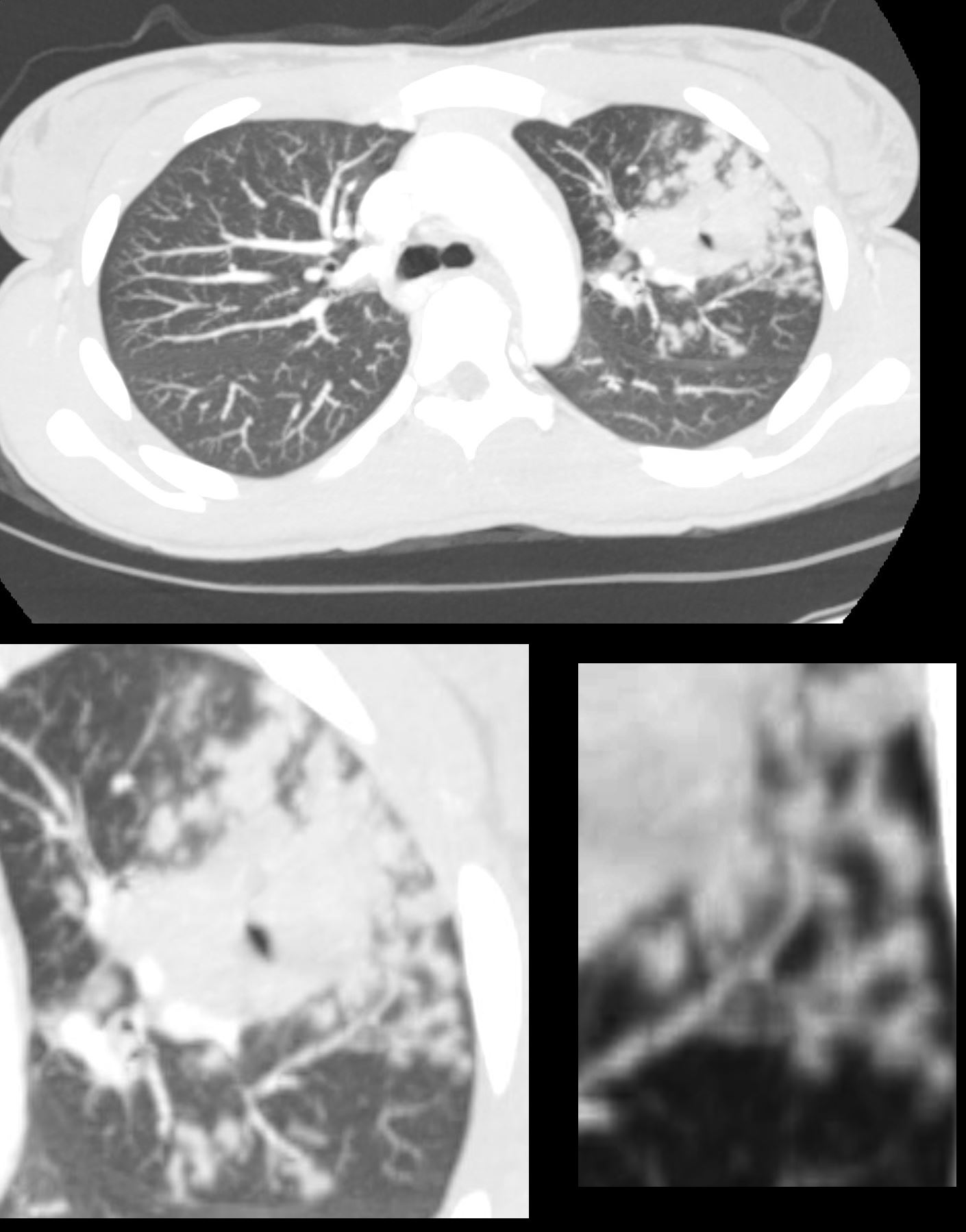
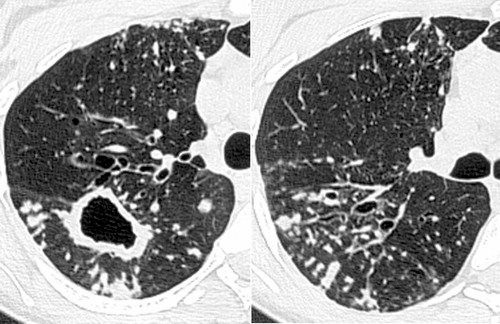
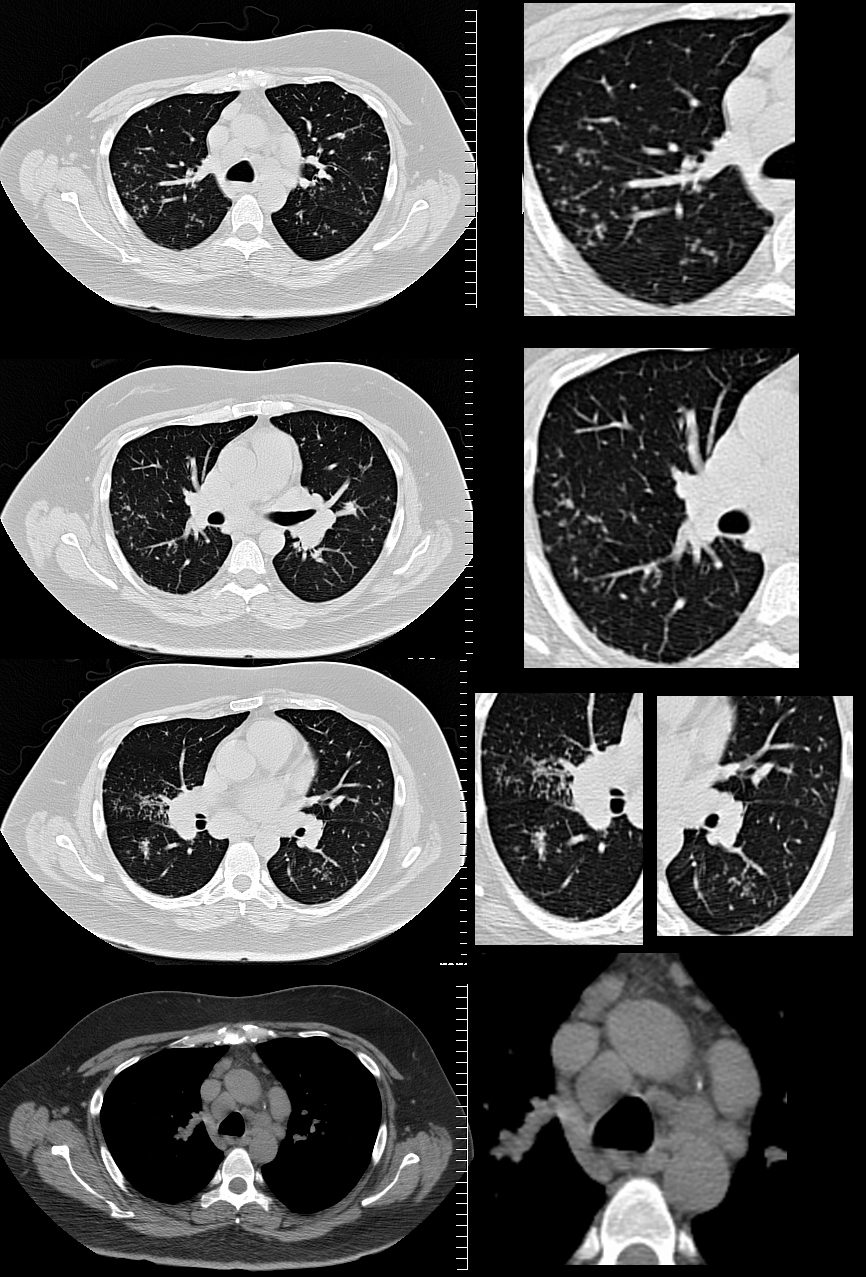
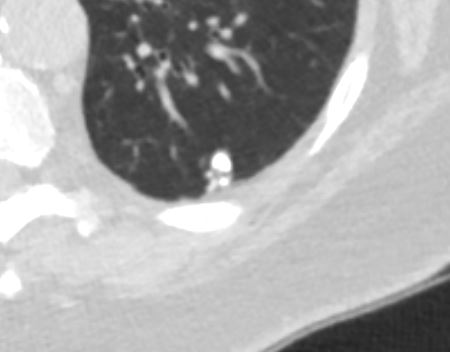
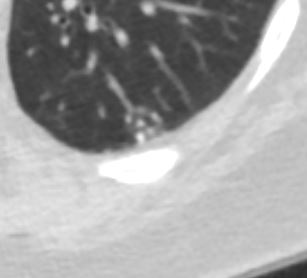
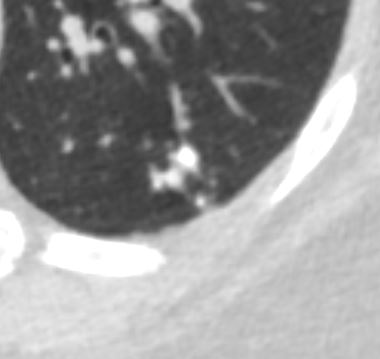
CT scan in the axial plane of the left upper lobe of a 28-year-old immigrant with cough shows a focal subsegmental consolidation with focal cavitation subtended by a thick-walled subsegmental airway. There are extensive tree in bud changes indicating transbronchial spread. Lab tests confirmed a diagnosis of TB and the patient was treated with RISE, a 4-month treatment regimen of rifapentine-moxifloxacin for mycobacterium tuberculosis.
Ashley Davidoff MD TheCommonVein.net 255Lu 136075c
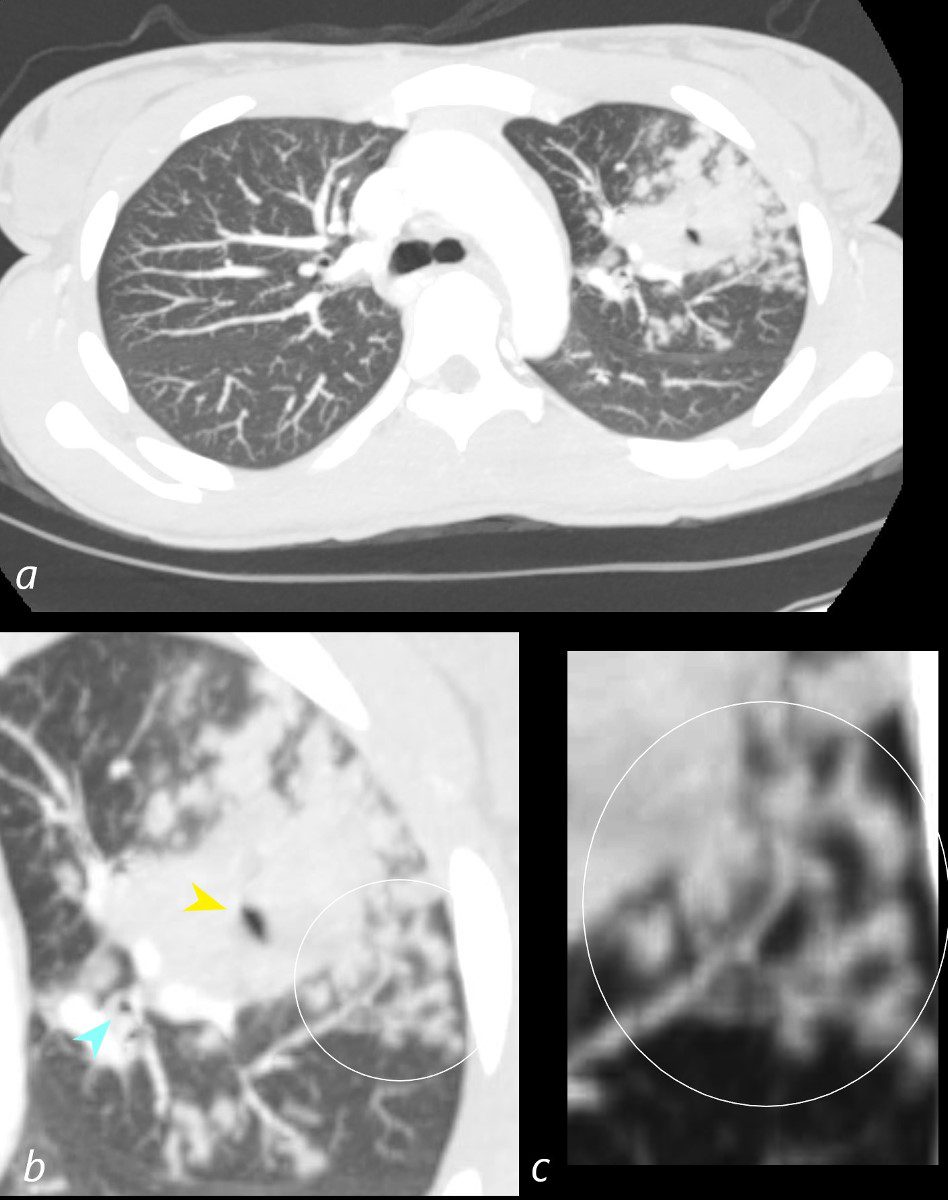
CT scan in the axial plane of the left upper lobe of a 28-year-old immigrant with cough shows a focal subsegmental consolidation with focal cavitation (yellow arrowhead) subtended by a thick-walled subsegmental airway. There are extensive tree in bud changes ringed in white (b and c) indicating transbronchial spread. Lab tests confirmed a diagnosis of TB and the patient was treated with RISE, a 4-month treatment regimen of rifapentine-moxifloxacin for mycobacterium tuberculosis.
Ashley Davidoff MD TheCommonVein.net 255Lu 136075cL
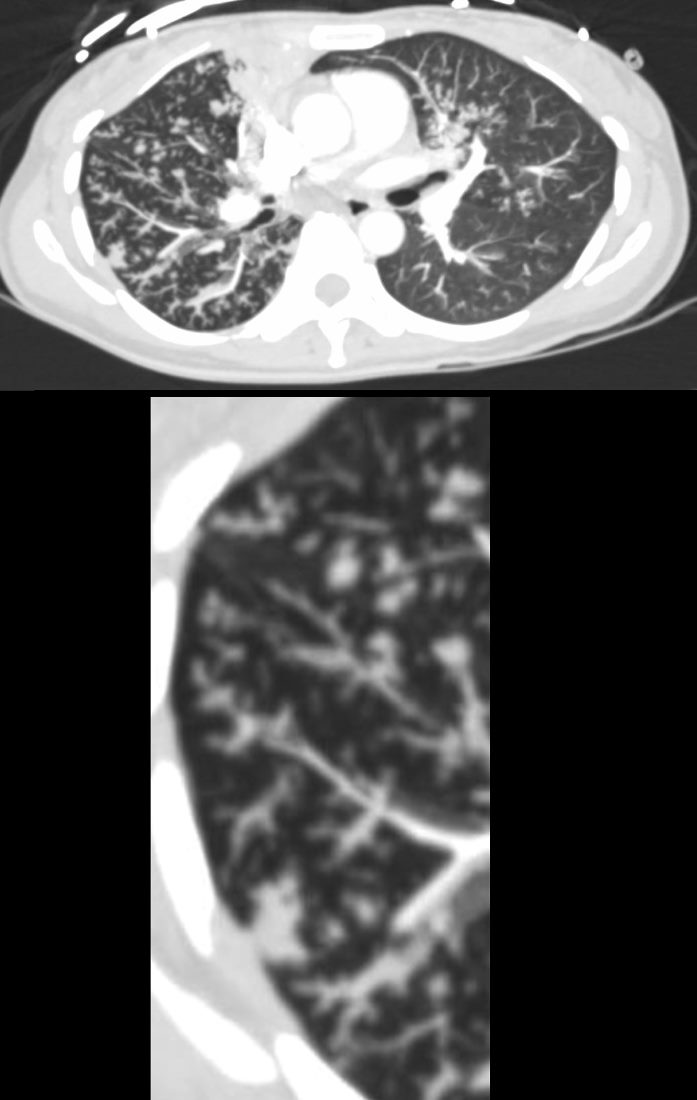
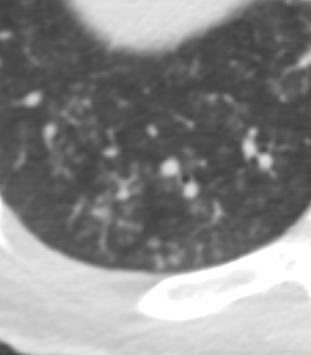
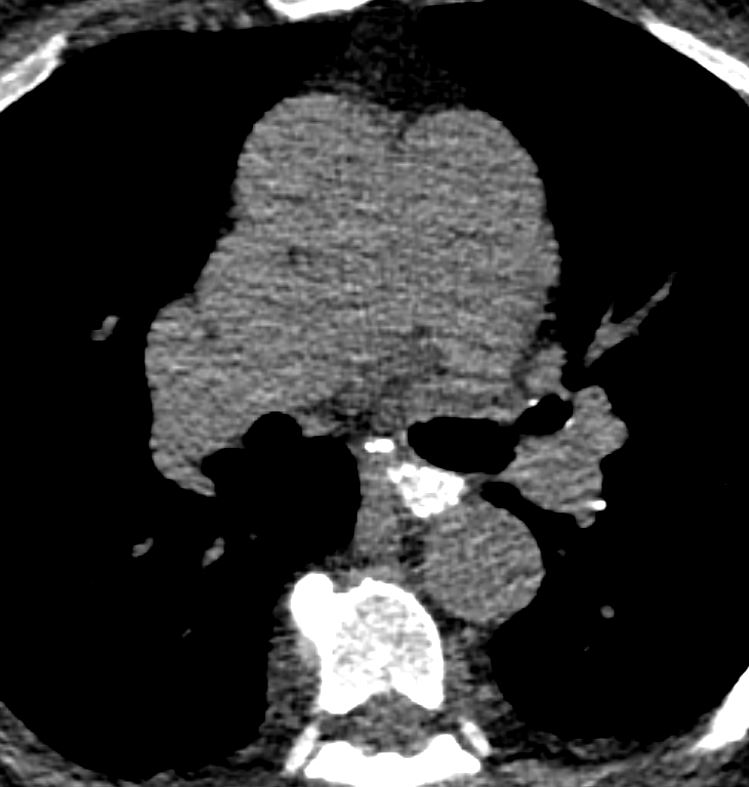
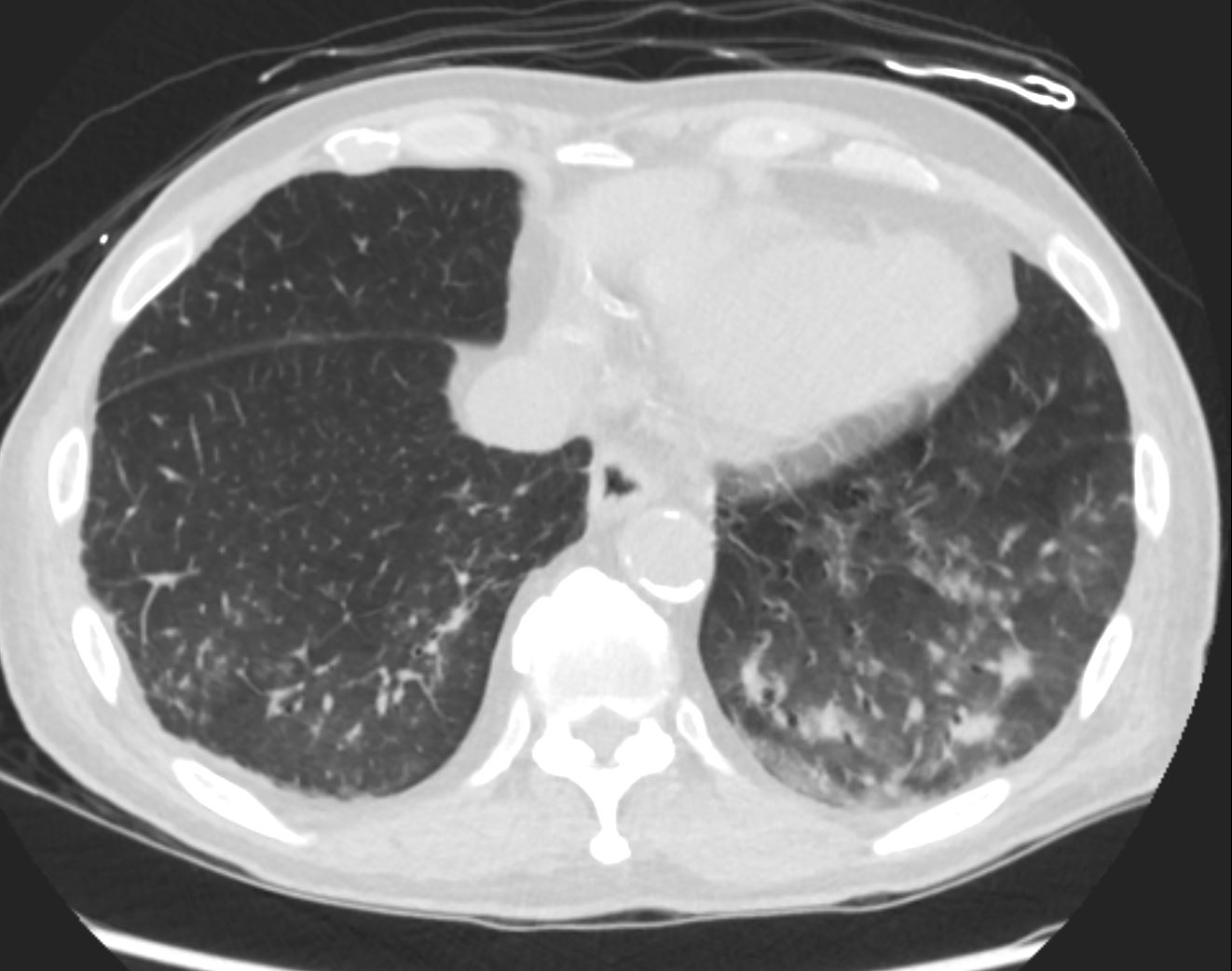
39-year-old immigrant Vietnamese male presents night sweats fever and cough. CT in the axial plane through the mid chest shows innumerable micronodules resulting from transbronchial spread with resultant tree in bud pattern.
Ashley Davidoff MD TheCommonvein.net 135788c 006Lu
Mycobacterium Avium Complex (MAC)
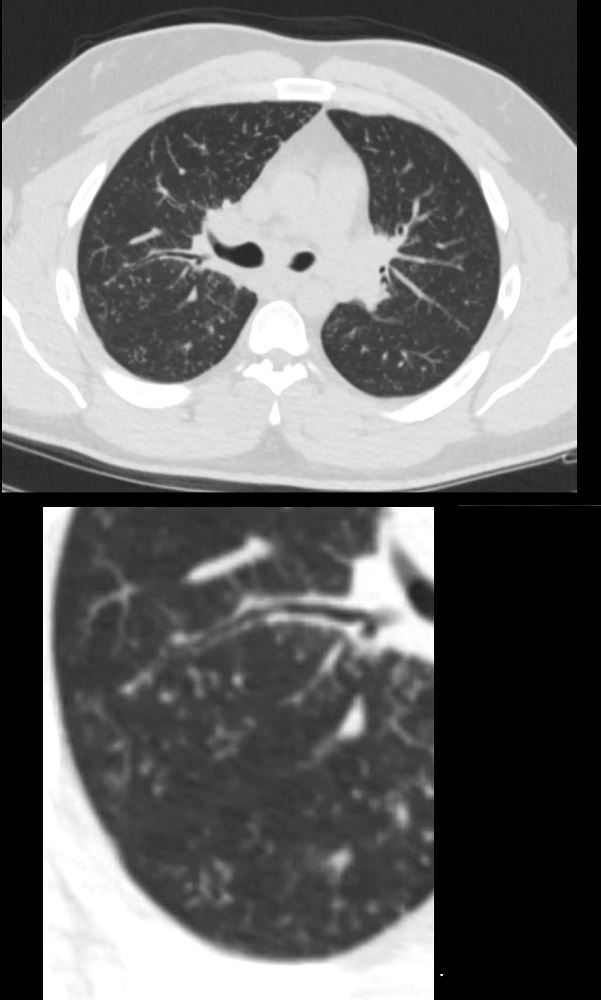
29-year-old male presents with night sweats
CT at the level of the carina shows extensive accumulation of ground glass micronodules and noted regions of tree in bud morphology. Wedge biopsy and culture revealed a diagnosis of MAC (mycobacterium avium complex)
Ashley Davidoff MD TheCommonvein.net 135813c 247Lu
Ashley Davidoff MD TheCommonVein.net
Aspergillus
Bronchopneumonic Form
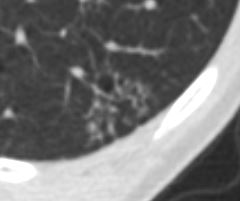
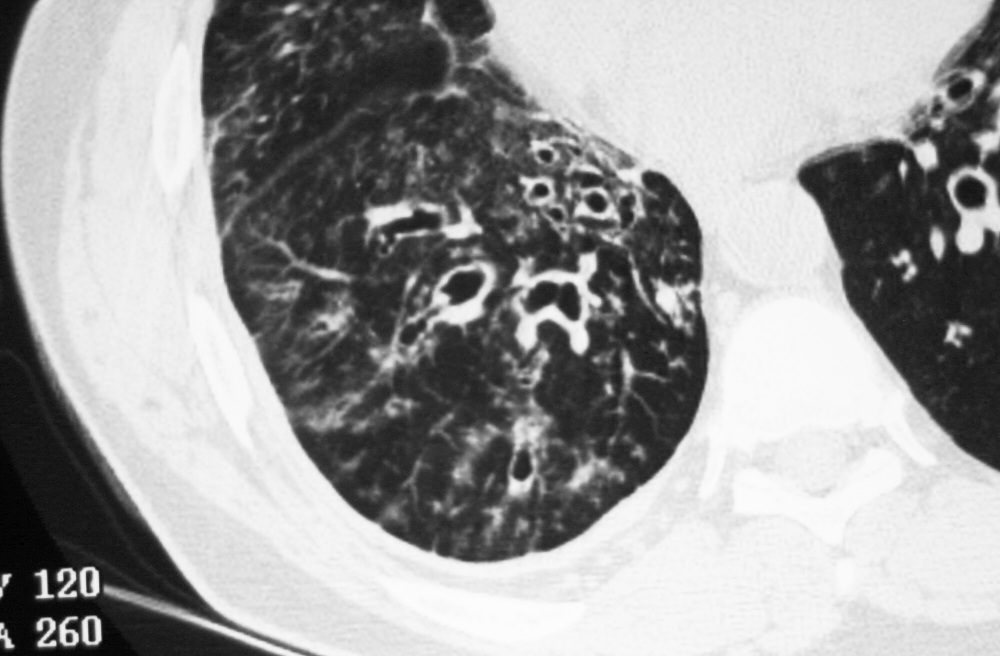
43 year old man with known aspergillus infection. Note the thickening of the walls of the segmental subsegmental and small airways with extensive tree in bud changes and bronchial wall thickening. There are centrilobular nodules indicating the small airway disease
Ashley Davidoff MD TheCommonVein.net
117816c
Axial Ct scan focused on the right lung base shows ground glass micronodules revealing a combination of centrilobular nodules and tree in bud sign indicating small airway disease
Diagnosis Aspergillus Infection
Ashley Davidoff TheCommonVein.net 219Lu-015
ABPA
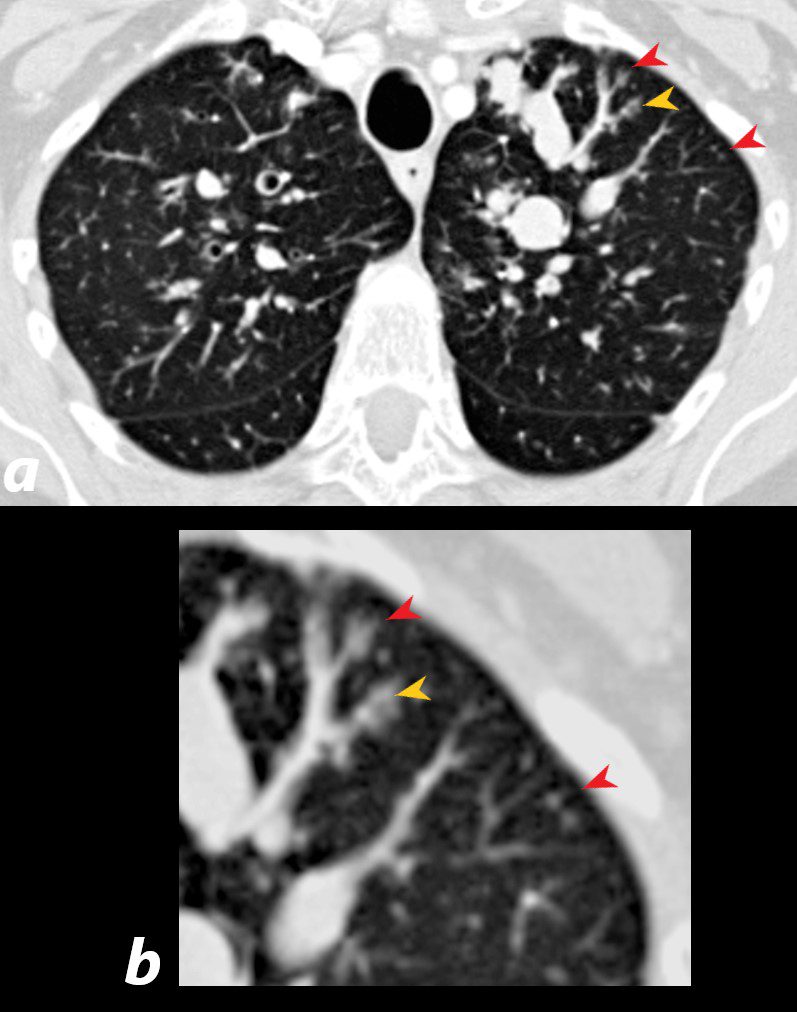
60 year old male with history of asthma, allergic bronchopulmonary aspergillosis (ABPA)
CT scan shows left upper lobe bronchiectasis and soft tissue/fluid impaction in the anterior segmental and subsegmental airways associated with tree in bud appearance (yellow arrowhead) and centrilobular nodules (red arrowhead) reminiscent of associated small airway disease
Ashley Davidoff TheCommonVein.net 221Lu 47113
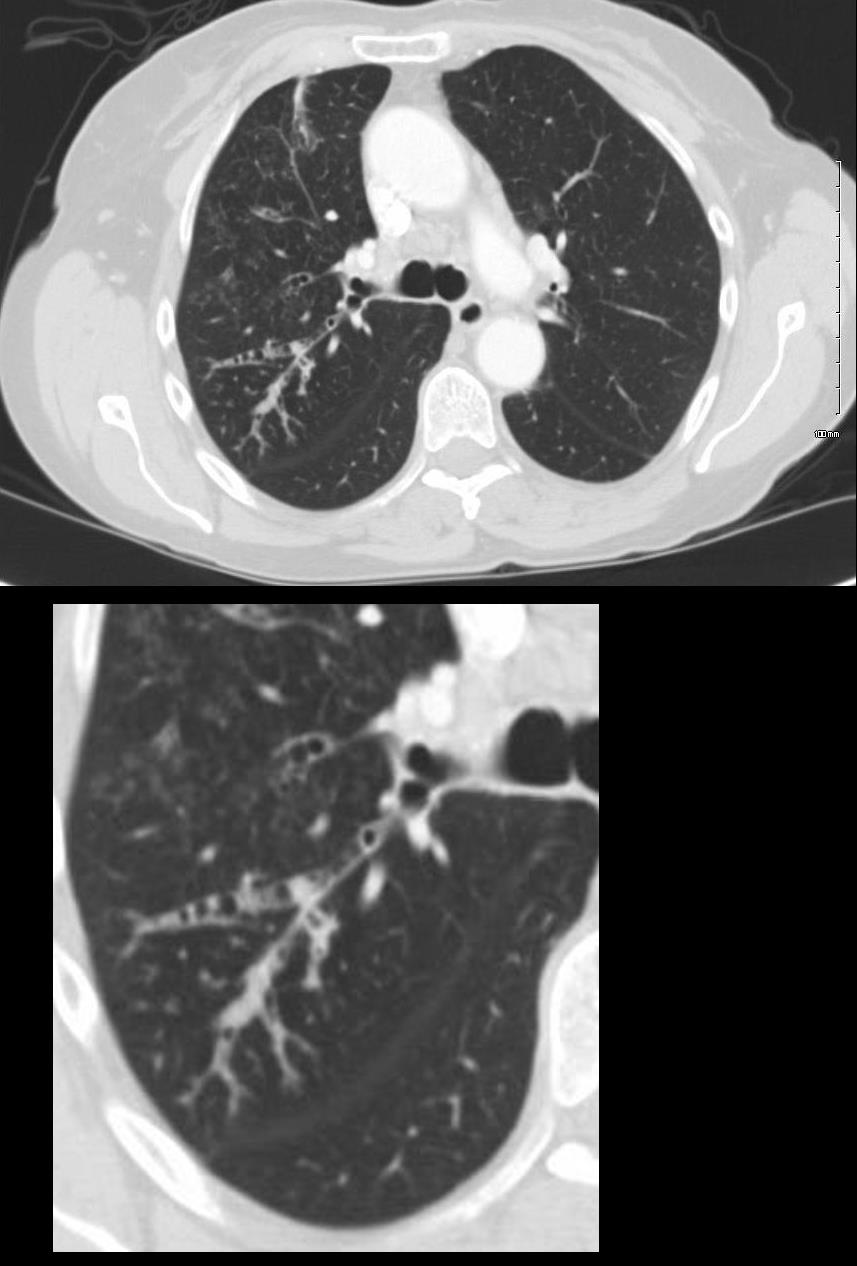
ABPA Current
CT Scan RUL
72 year old female with asthma with cough and chronic dyspnea.
CT in the axial plane shows thickening of the segmental and subsegmental airways of the posterior segment of the right upper lobe with mucoid impaction and tree in bud formation
Ashley Davidoff MD TheCommonVein.net 294Lu 117967c
Bronchiectasis
CT af the right lung base shows thickening and bronchiectasis of the segmental and subsegmental airways with extension to the small airways showing bronchiolectasis and tree in bud morphology
Ashley Davidoff MD TheCommonVein.net 31744
HP
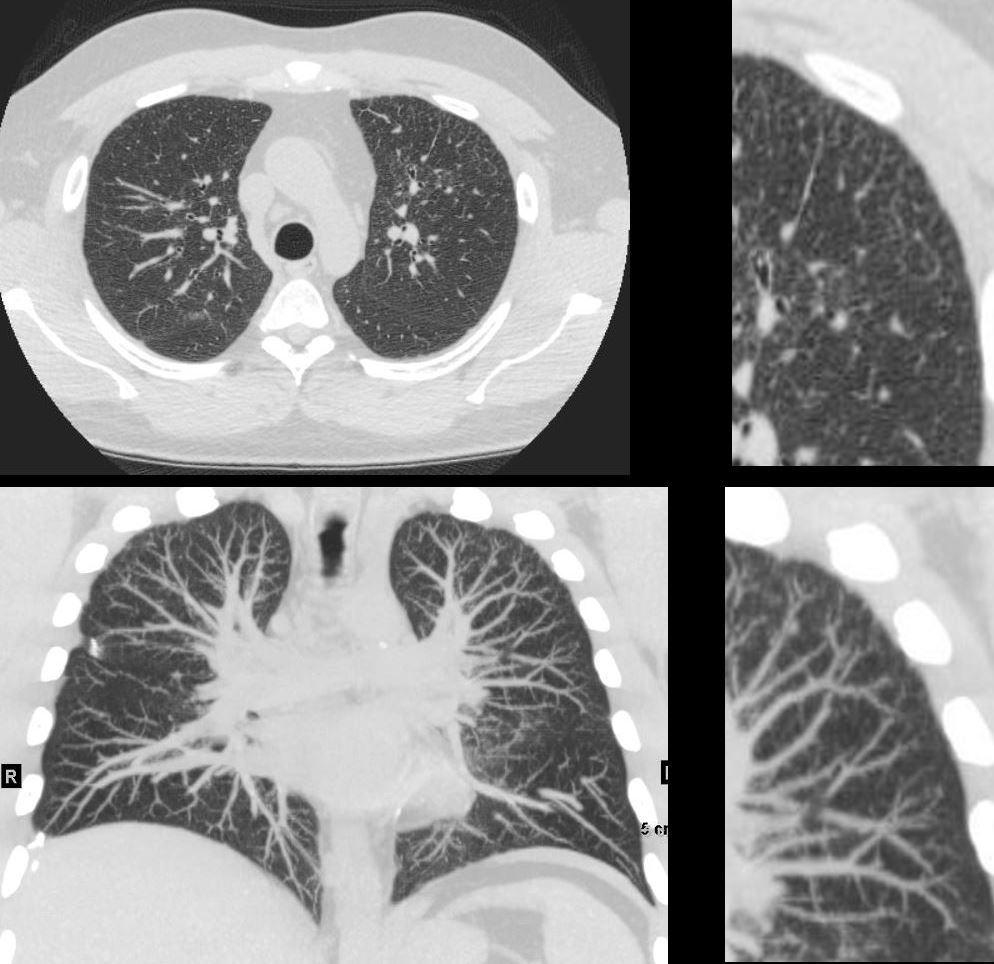
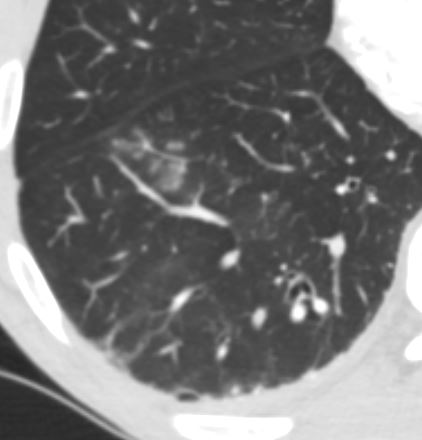
CT in the axial (upper)and coronal plane (lower panels) show most prominent changes in the anterior segment of the left upper lobe
The findings are characterized and best appreciated in the upper right panel by evidence of small airway disease including tree in bud and centrilobular nodules most prominent in the periphery
Ashley Davidoff MD TheCommonVein.net 135835
CT in the axial (upper)and coronal plane (lower panels) show most prominent changes in the anterior segment of the left upper lobe
The findings are characterized and best appreciated in the upper right panel by evidence of small airway disease including tree in bud and centrilobular nodules most prominent in the periphery
Ashley Davidoff MD TheCommonVein.net 135835
Aspiration
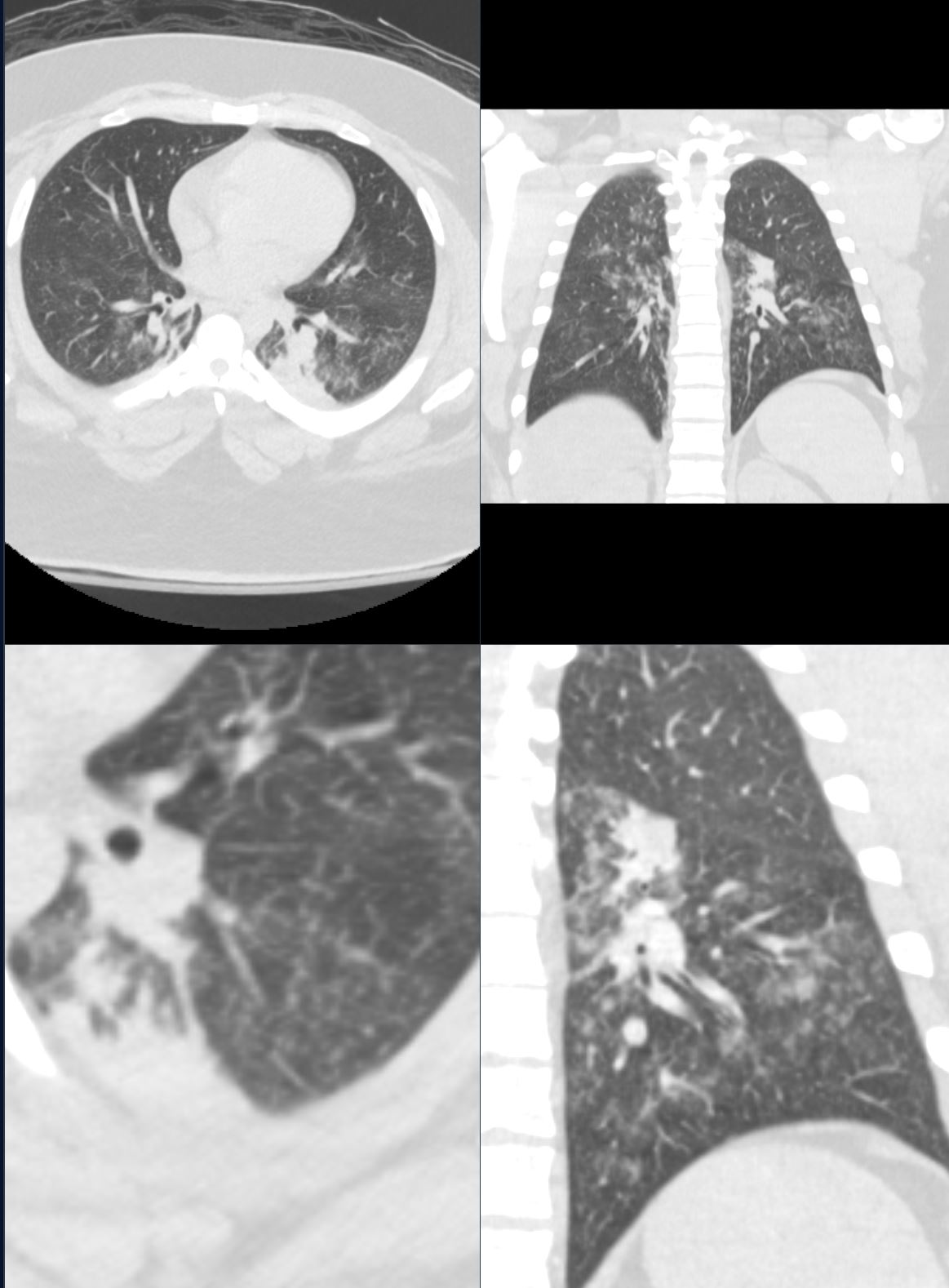
Patient presents with acute dyspnea
CT scan shows segmental atelectasis in the left lower lobe associated with filling of the bronchi and small airways with tree in bud morphology consistent with a diagnosis of aspiration
Ashley Davidoff MD TheCommonVein.net b11818
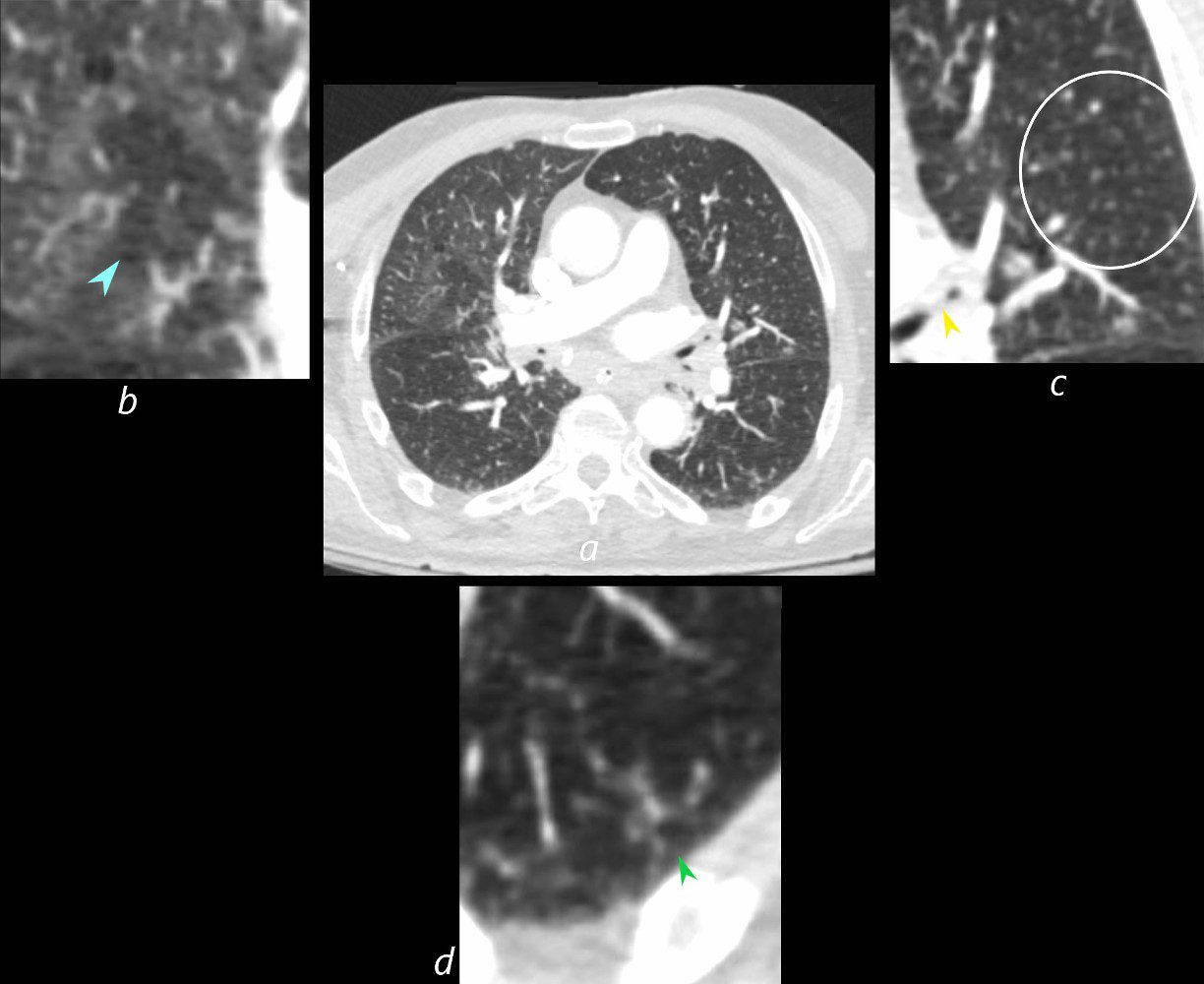
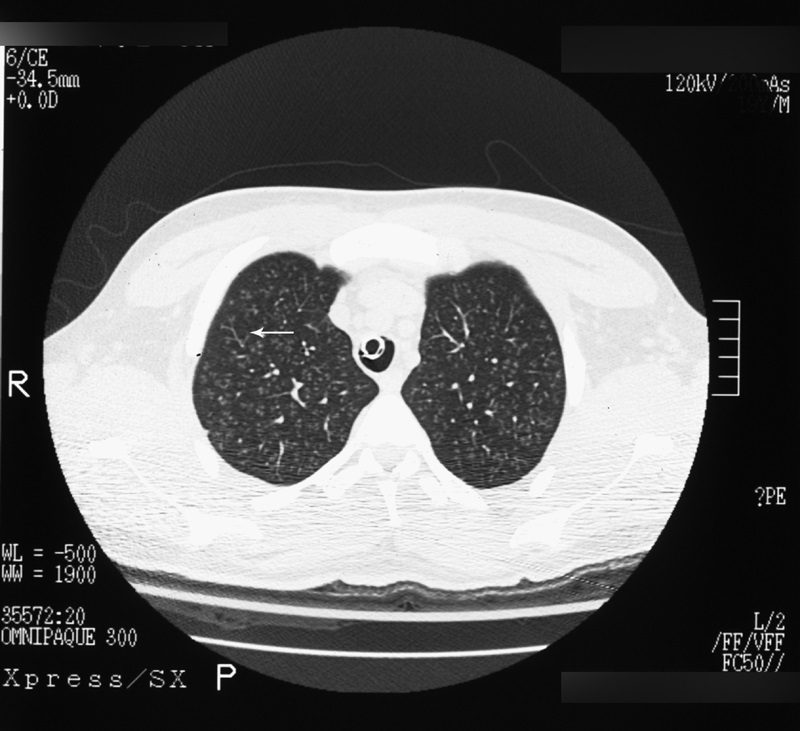
73-year-old man presents with respiratory difficulty following trauma and difficult placement of a nasogastric tube. CT scan through the upper chest at the level of the right pulmonary artery shows a focus of mosaic attenuation in the right upper lobe with a central vasoconstricted vessel (b blue arrowhead). The left upper lobe bronchus contains aspirated material (c yellow arrowhead) and there are multiple ill-defined micronodules (b, white circle). The left lower lobe shows peripheral tree in bud nodularity (d green arrowhead). In the clinical context of technical difficulty with a recently placed NG tube acute, aspiration of fluid gastric content with small airway involvement is a diagnostic consideration despite the lack of alveolar changes
Ashley Davidoff MD TheCommonVein.net 135762cL
43 year female found unconscious CT showed finding in the posterior segment of the right upper lobe and consolidation and tree in bud changes reflecting acute aspiration pneumonia
Ashley Davidoff MD TheCommonVein.net consolidation pneumonia aspiration-43f004-ct-tree-in-bud
Differential Diagnosis
Conditions that may mimic the tree-in-bud sign include:
- Miliary Nodules:
- Random distribution, not branching.
- Vascular Disease:
- Centrilobular vascular opacities (e.g., pulmonary hemorrhage).
- Sarcoidosis:
- Perilymphatic distribution of nodules rather than centrilobular.
Clinical Significance
- The Tree-in-Bud sign indicates a small airway disease, often with infectious or inflammatory pathology.
- It is important to correlate the radiological findings with clinical symptoms (e.g., cough, fever, dyspnea) and laboratory tests (e.g., sputum culture, serology).
Imaging Modalities
- High-Resolution CT (HRCT):
- Gold standard for identifying and characterizing the TIB sign.
- Chest X-Ray:
- Often non-specific and may miss subtle airway pathology.

Ashley Davidoff
TheCommonVein.net
Ashley Davidoff MD The CommonVein.net
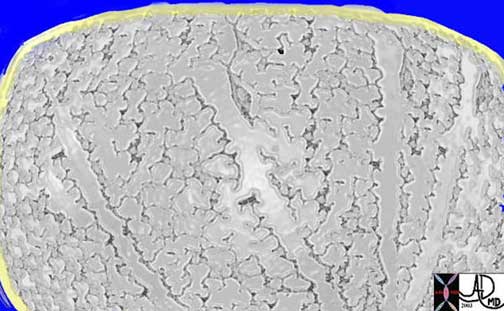 Respiratory bronchioles, alveolar sacs, and alveoli
Respiratory bronchioles, alveolar sacs, and alveoli
This drawing shows about 3-4 respiratory bronchioles that serve to make a secondary lobule. Alveolar sacs and individual alveoli are also seen. The yellow border represents the visceral pleura on the surface.
Courtesy of: Ashley Davidoff, M.D.
Infection
- small (2–4-mm) centrilobular nodules and
- branching linear opacities of similar caliber
- originating from a single stalk
- bronchial wall thickening with or without
- bronchiectasis.
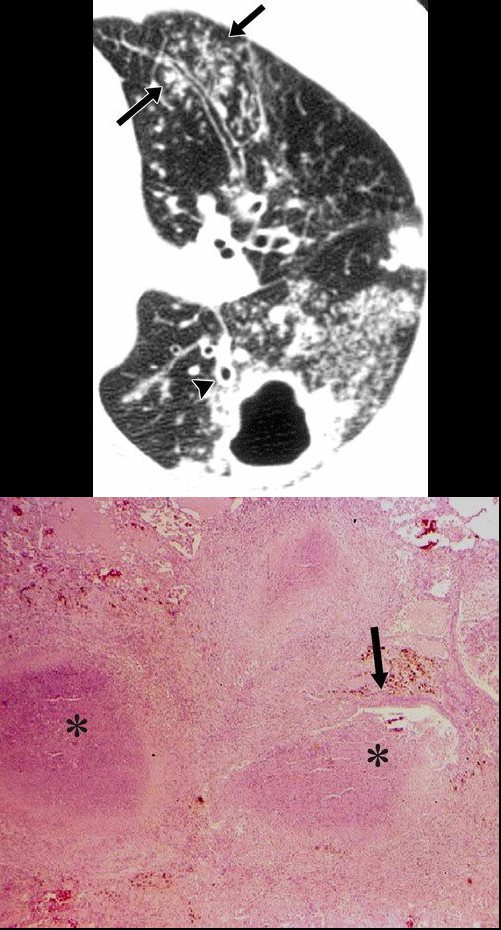
- Active TB
-

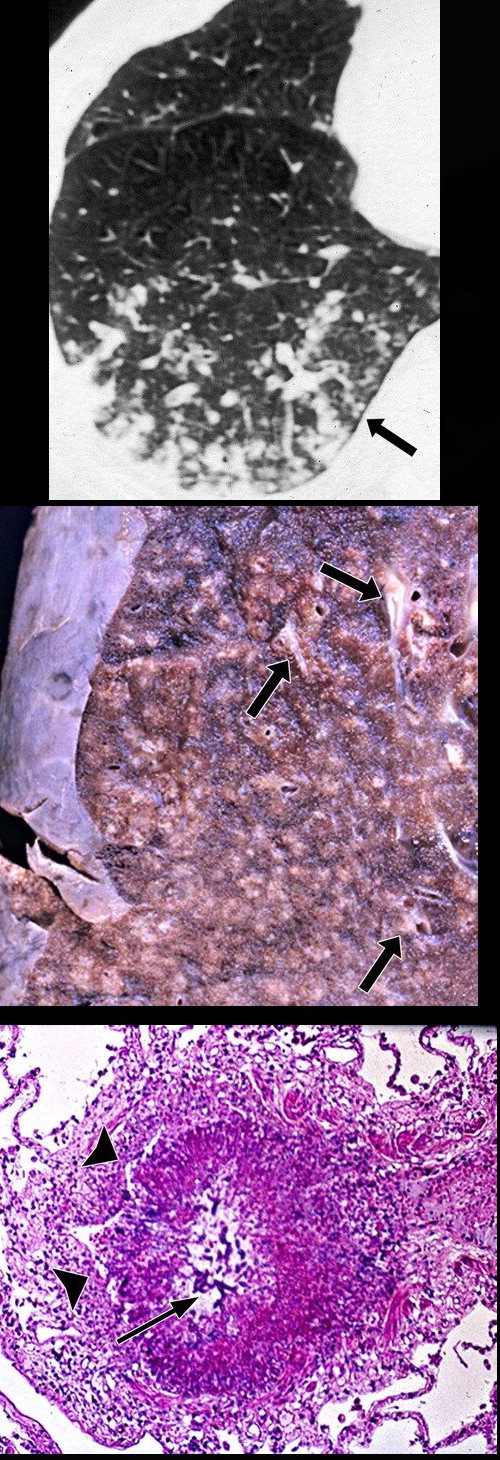
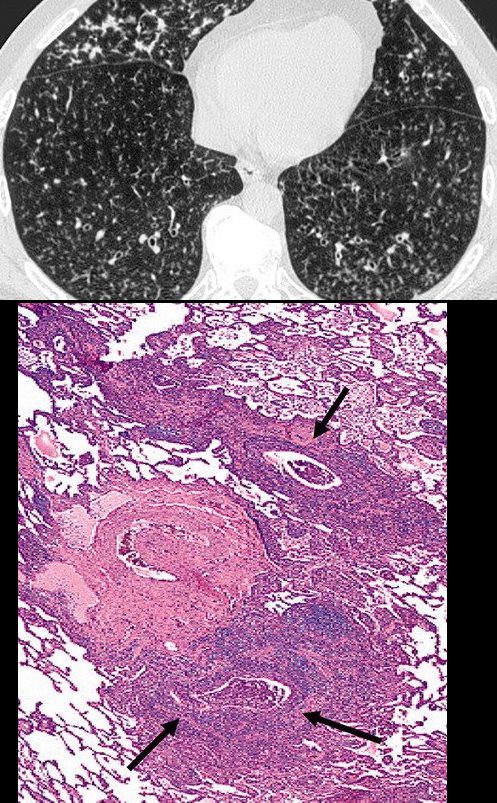
Postprimary active tuberculosis in a 34-year-old man with weight loss and a chronic cough. (a) High-resolution CT scan of the left lung shows a thick-walled cavity and multiple peripheral small nodules and branching linear structures (arrows). Note the thickening of the bronchial walls (arrowhead). (b) Photomicrograph (original magnification, ×400; hematoxylin-eosin stain) shows impacted caseous material (*) in small peripheral airways (arrow).
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005 - TB
-
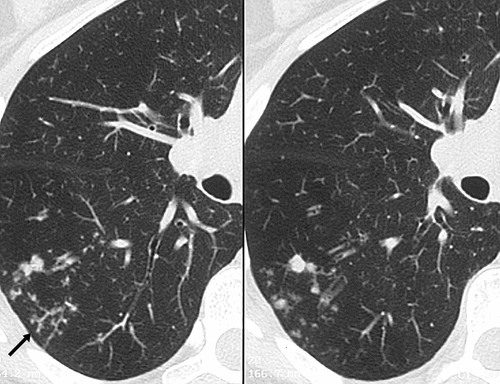
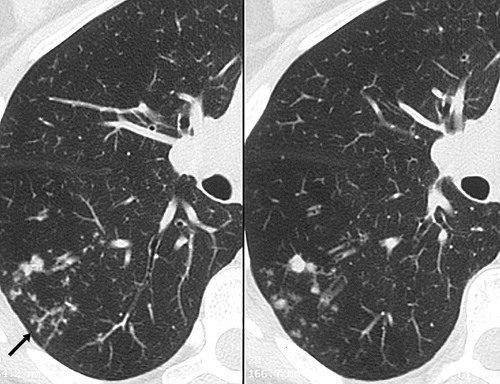
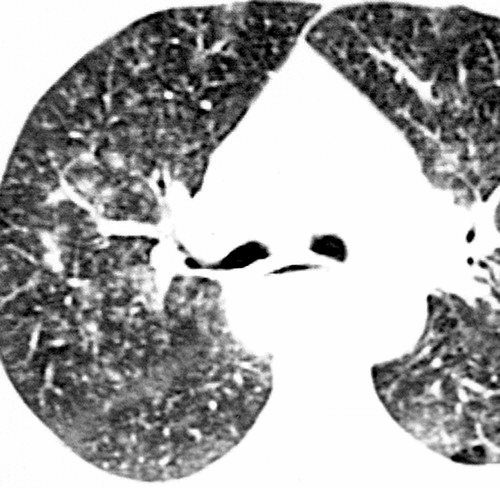
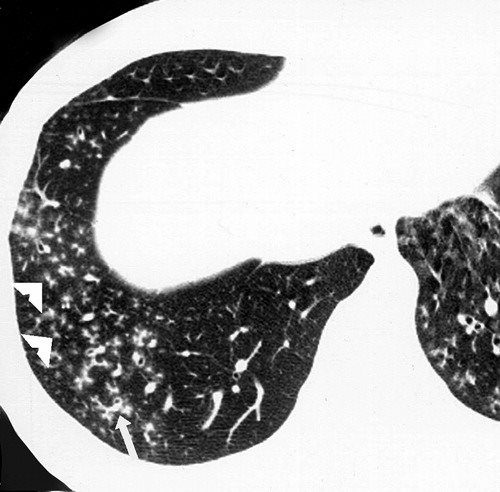
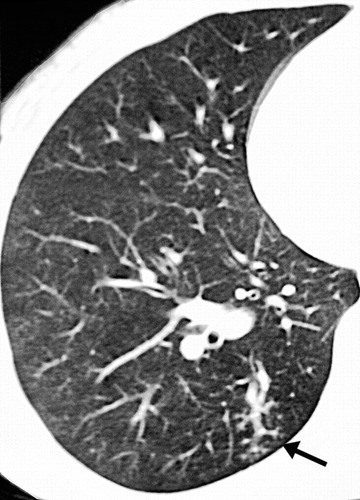
Post primary active tuberculosis in a 66-year-old woman with a chronic cough. High-resolution CT scans of the right lung show peripheral, poorly defined, small (2–4-mm-diameter) centrilobular nodules and branching linear opacities of similar caliber originating from a single stalk (the tree-in-bud pattern) in the lower lobe (arrow). These findings represent endobronchial spread of tuberculosis.
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005Postprimary active tuberculosis in a 66-year-old woman with a chronic cough. High-resolution CT scans of the right lung show peripheral, poorly defined, small (2–4-mm-diameter) centrilobular nodules and branching linear opacities of similar caliber originating from a single stalk (the tree-in-bud pattern) in the lower lobe (arrow). These findings represent endobronchial spread of tuberculosis.
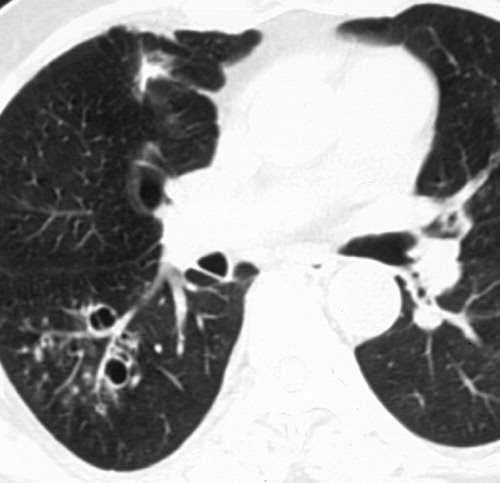
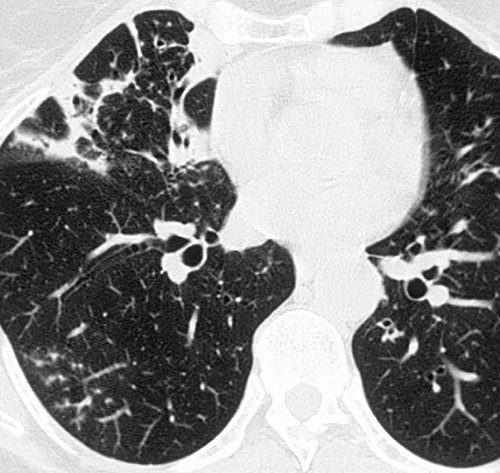
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005Infection with M avium-intracellulare complex in a 44-year-old woman with malaise and a chronic cough. High-resolution CT scans of the right lung show multiple peripheral small nodules connected to branching linear opacities and a thick-walled cavity in the superior segment of the lower lobe. Note the thickening of the bronchial walls, bronchial dilatation, and mucus impaction. The diagnosis was confirmed with bronchoalveolar lavage.
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005 - Aspergillus and Tree in Bud Sign
CT scan through the chest shows medium sized bronchi, bronchioles and small airways impacted with fluid. This collage is presented to reveal tree in bud changes resulting from impaction in the smaller terminal bronchioles and respiratory units. The tree-in-bud pattern also results in small centrilobular nodules connected to multiple branching linear structures of similar caliber from a single stalk. Originally it was felt to result from endobronchial spread of Mycobacterium tuberculosis, but is is now recognized in diverse entities including peripheral airway diseases caused by infection (bacterial, fungal, viral, or parasitic), congenital disorders, idiopathic disorders (obliterative bronchiolitis, pan bronchiolitis), aspiration or inhalation of foreign substances, immunologic disorders, connective tissue disorders and peripheral pulmonary vascular diseases such as neoplastic pulmonary emboli.
In this case there are also dilated medium sized airways, impacted with soft tissue characteristic of the finger in glove sign and most likely due to allergic bronchopulmonary aspergillosis (ABPA)
Ashley Davidoff MD Ashley Davidoff MD TheCommonVein.net
47113c01
43 year old man with known aspergillus infection. Note the thickening of the walls of the segmental subsegmental and small airways with extensive tree in bud changes and bronchial wall thickening. There are centrilobular nodules indicating the small airway disease
Ashley Davidoff MD TheCommonVein.net
117816c
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
Other Infections
Staphylococcus Aureus
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
Hemophilus Influenza
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
CMV
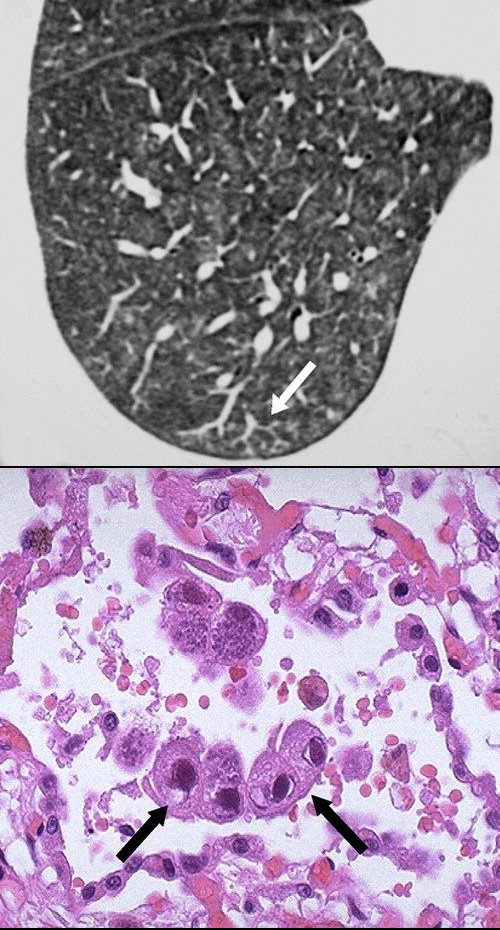
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
Respiratory Syncytial Virus

Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
87 year old male with history of cough and suspicion of aspiration shows barium aspiration into the proximal trachea (upper right) The scout view ( upper right) shows an infiltrate at the right base, Thickened airways in the right lower lobe (2nd row left ) is associated with a pneumonic infiltrate in the right lower lobe (lower right) consistent with aspiration. There are thickened airways to the lingula (3rd and 4th row) with magnified view showing tree in bud changes (right sided images 3rd and 4th row)
These findings likely relate to infection, often fungal or granulomatous
Ashley Davidoff MD Ashley Davidoff MD TheCommonVein.net
Inflammatory Diseases
Aspiration and Tree in Bud
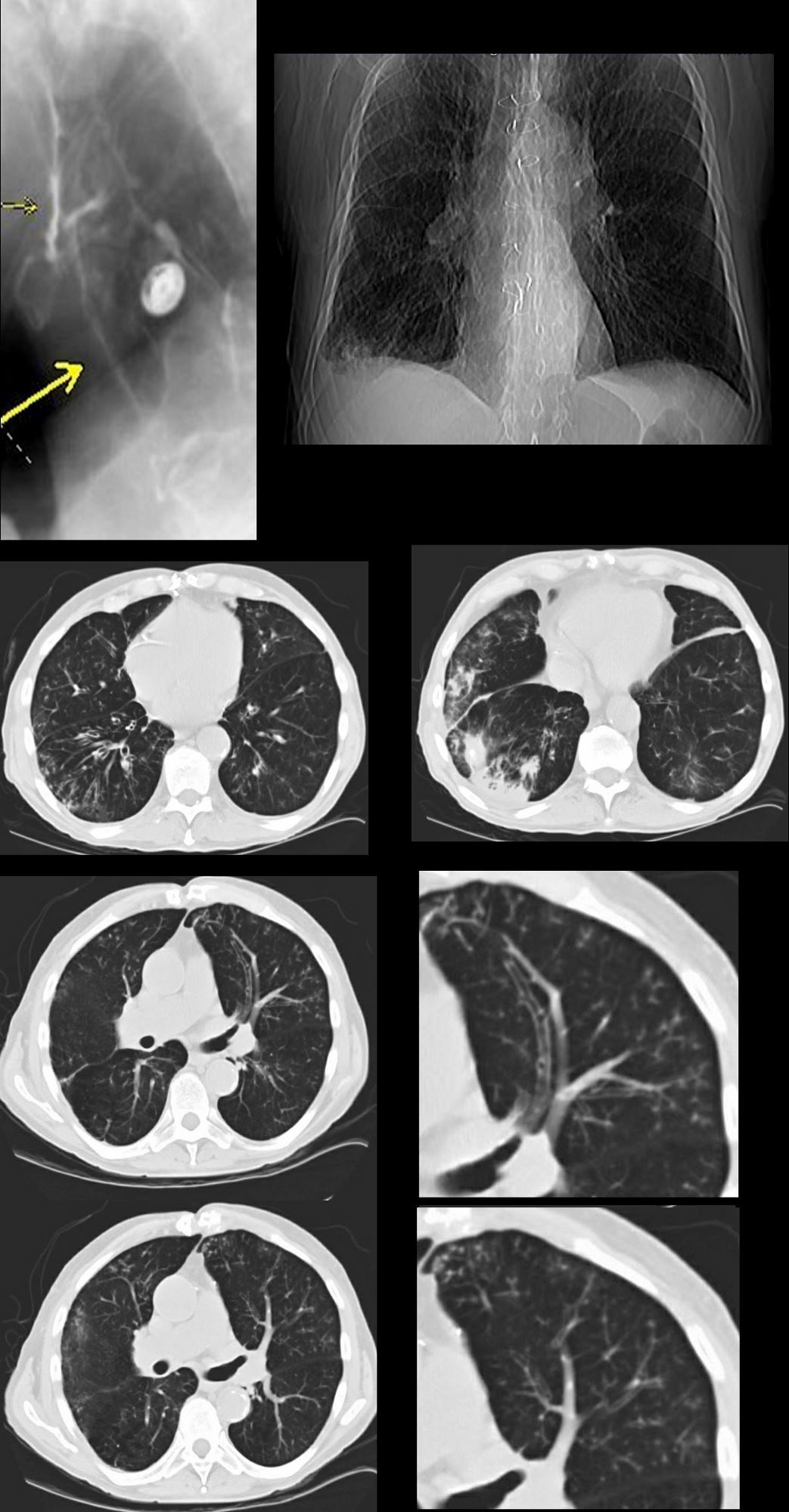
87 year old male with history of cough and suspicion of aspiration shows barium aspiration into the proximal trachea (upper right) The scout view ( upper right) shows an infiltrate at the right base, Thickened airways in the right lower lobe (2nd row left ) is associated with a pneumonic infiltrate in the right lower lobe (lower right) consistent with aspiration. There are thickened airways to the lingula (3rd and 4th row) with magnified view showing tree in bud changes (right sided images 3rd and 4th row)
All these finding likely relate to aspiration though lingula involvement is not usual
Ashley Davidoff MD Ashley Davidoff MD TheCommonVein.net
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
Asthma

55F-asthma-involving medium and small sized airways focal consolidations and chronic sinusitis with tree in bud
Ashley Davidoff TheCommonVein.net
Inhalation Bronchiolitis
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
Obliterative Bronchiolitis aka (bronchiolitis obliterans is also known and constrictive bronchiolitis) association to lung transplant and bone marrow transplant
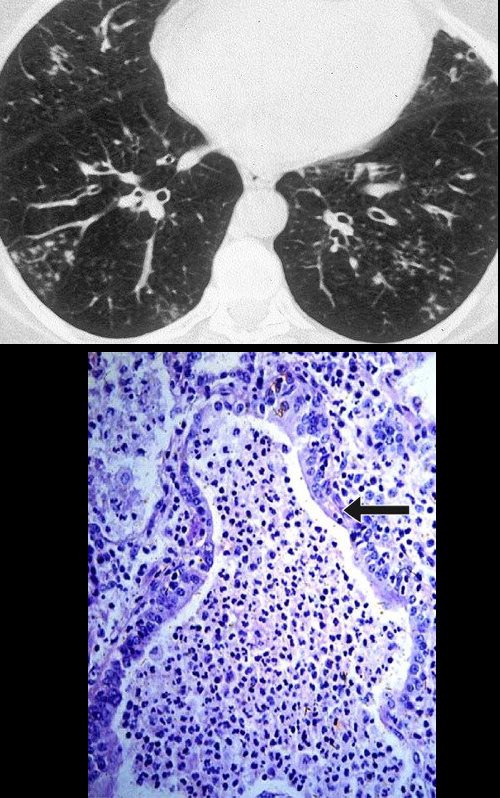
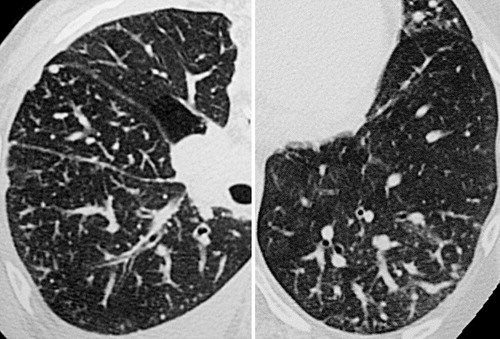
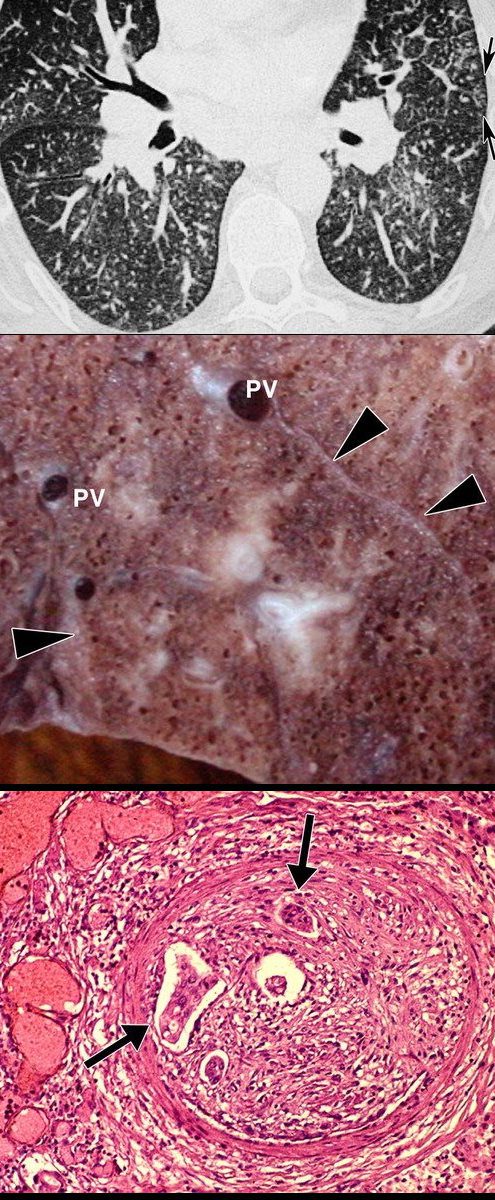
Obliterative bronchiolitis after bone marrow transplantation in a 47-year-old man with myeloma. (a) Expiratory high-resolution CT scan shows diffuse centrilobular nodules connected to branching linear opacities bilaterally. Note the air trapping in the right lower lobe. (b) Photomicrograph (original magnification, ×200; hematoxylin-eosin stain) of a specimen from open lung biopsy shows the bronchiolar walls surrounded by concentric chronic inflammatory infiltrates (arrows).
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
Circulatory
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
Rossi, SE et al Tree-in-Bud Pattern at Thin-Section CT of the Lungs: Radiologic-Pathologic Overview RadioGraphics Vol. 25, No. 3 2005
Tree in Bud with
Ashley Davidoff MD TheCommonVein.net
Source
Signs in Thoracic Imaging
Journal of Thoracic Imaging 21(1):76-90, March 2006.
https://pubs.rsna.org/doi/full/10.1148/radiol.13120908
Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net

Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net
Ashley Davidoff
TheCommonVein.net

Ashley Davidoff MD TheCommonvein.net
Ashley Davidoff MD TheCommonvein.net
- Parallels with Human Endeavors
- Examples in Social and Societal Equivalents
- The tree-in-bud pattern mirrors spring’s renewal, symbolizing a mix of growth and obstructions along pathways.
- The branching opacity highlights the tension between vitality and impairment, much like life cycles where struggles precede renewal.
- Art: The tree-in-bud pattern is reminiscent of blossoming trees depicted in classical spring paintings.
- Examples in Social and Societal Equivalents
 Le Printemps (Springtime). Monet, Claude (French, 1840-1926). Oil on canvas, 1886. Purchased With a contribution from the National Art Collections Fund.
Le Printemps (Springtime). Monet, Claude (French, 1840-1926). Oil on canvas, 1886. Purchased With a contribution from the National Art Collections Fund.
Sculpture: Branching structures in sculptures symbolize interconnectedness and growth.
Le_Printemps 1911 – Aristide_Maillol
Spring

Music: Melodic compositions with branching motifs reflect renewal and progression.

Dance: Movements echoing budding and branching represent spring’s energy.
Mark Morris Dance Group Spring, Spring, Spring

Chinese Traditional Dancing – Recall That Spring

Literature: Spring often symbolizes new beginnings and the resolution of blockages.
Shakespeare
Henry VI, Part II
Now ’tis the spring, and weeds are shallow-rooted;
Suffer them now, and they’ll o’ergrow the garden
Quotes by famous people: “Spring is nature’s way of saying, ‘Let’s party!'” — Robin Williams.
Poetry: Poems often compare spring’s renewal to life’s potential.
Architecture: Designs inspired by trees, such as branching structures, signify resilience and connection.
References and Links
Miller WT, Panosian JS. Chest. 2013;144(6):1883-1892. doi:10.1378/chest.13-1270.
Li Q, Fan X, Huang XT, et al. Lung Cancer (Amsterdam, Netherlands). 2015;88(3):260-6. doi:10.1016/j.lungcan.2015.03.009.
4.Tree-in-Bud Pattern of Pulmonary Tuberculosis on Thin-Section CT: Pathological Implications. Im JG, Itoh H. Korean Journal of Radiology. 2018 Sep-Oct;19(5):859-865. doi:10.3348/kjr.2018.19.5.859.
Terhalle E, Günther G. Respiration; International Review of Thoracic Diseases. 2015;89(2):162-5. doi:10.1159/000370050.