

Ashley Davidoff MD TheCommonvein.net lungs-0774
- Common reasons
-
- Larger volume
- Gravity
- Increased oxygen tension
- increase oxidative stress
- Increased lymphatics
- Decreased perfusion
- Gas exchange is more efficient in the lower lobes
- Blood Flow is higher in the lower lobes
-
- Inhalational
- Centrilobular emphysema.
- TB
- InhaledParticlates
- Silicosis
- Berylliosis
- Pneumoconnioses
- Hypersensitivity Pneumonitis
- Allergic Bronchopulmonary Aspergillosis
- Sarcoidosis
- Langerhans Cell Histiocytosis
- Bronchocentric Granulomatosis
- Chronic Eosinophilia
- (peripheral and upper lobes)
- Cocaine
- Adenocarcinoma
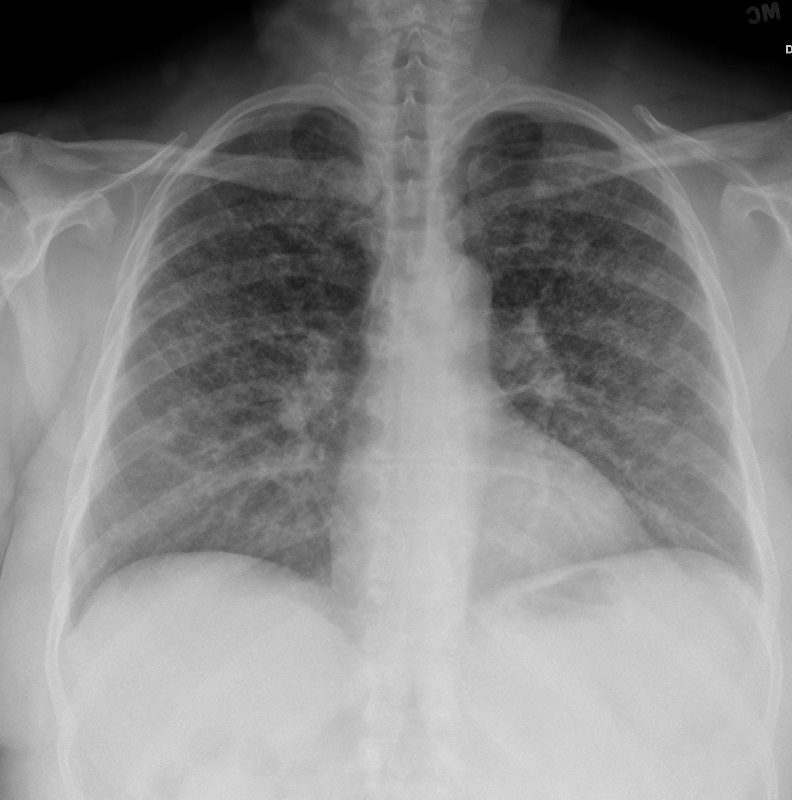
TB
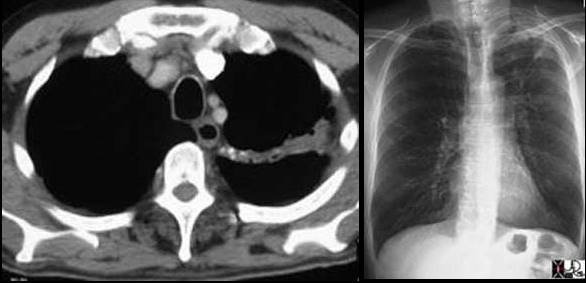 Left image: In this patient with TB there is a linear band like density with calcifications in the LUL characteristic of atelectatic change in the LUL. This loss of volume is associated with fibrosis and retraction seen on the CXR in the following image. Courtesy of: Ashley Davidoff, M.D.
Left image: In this patient with TB there is a linear band like density with calcifications in the LUL characteristic of atelectatic change in the LUL. This loss of volume is associated with fibrosis and retraction seen on the CXR in the following image. Courtesy of: Ashley Davidoff, M.D.
Sarcoidosis

The CXR shows an interstitial process involving the upper lobecharacterised by a reticular pattern
Ashley Davidoff MD TheCommonvein.net lungs sarcoid 001

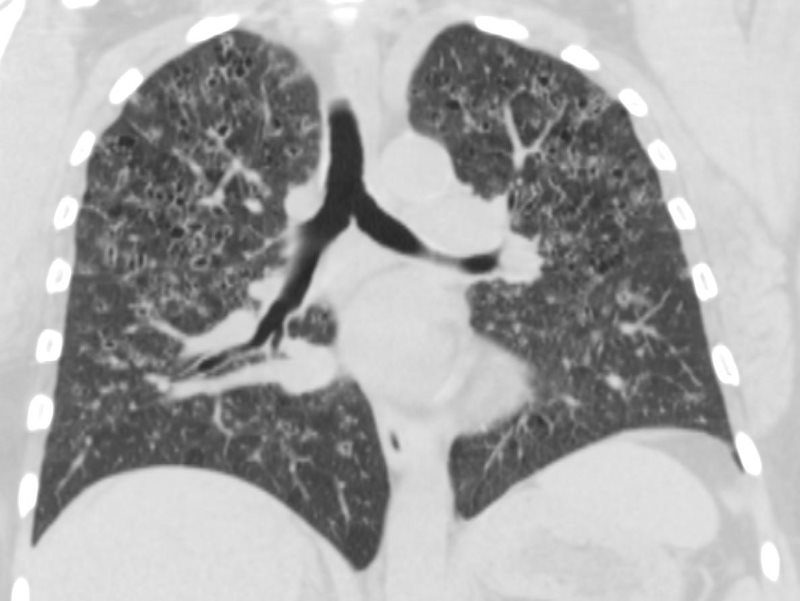
The coronal CTscan shows an interstitial with thickening and displacement of the fissure and innumerable micronodules some centrilobular and some related to the pleura
Ashley Davidoff MD TheCommonvein.net lungs sarcoid 004
The axial CTscan shows thickening and irregularity of the major fissure, a band of fibrosis in the right upper lobe, thickening of a segmental bronchus in the right upper lobeand bronchocentric fibrosis in the left upper lobeand multiple micronodules
Ashley Davidoff MD TheCommonvein.net lungs sarcoid 002
The axial CTscan shows an interstitial innumerable micronodules some centrilobular and some related to the pleura and others probably in the interlobular septa (posterior right upper lobe)
Ashley Davidoff MD TheCommonvein.net lungs sarcoid 003

SARCOIDOSIS vs SILICOSIS
42-year-old cement worker presents with dyspnea .
A CXR performed 5 years prior was close to normal with possible right hilar prominence.
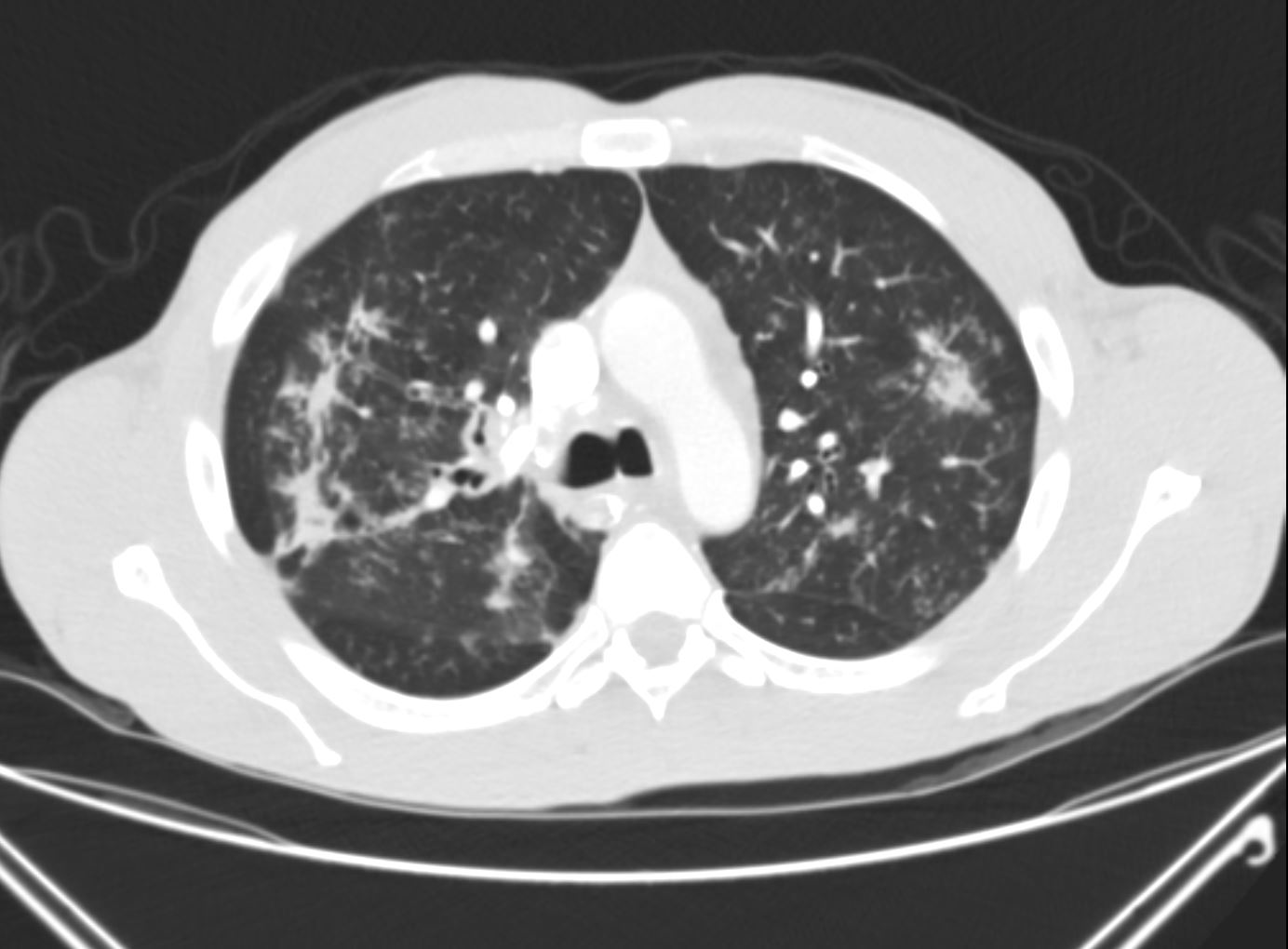
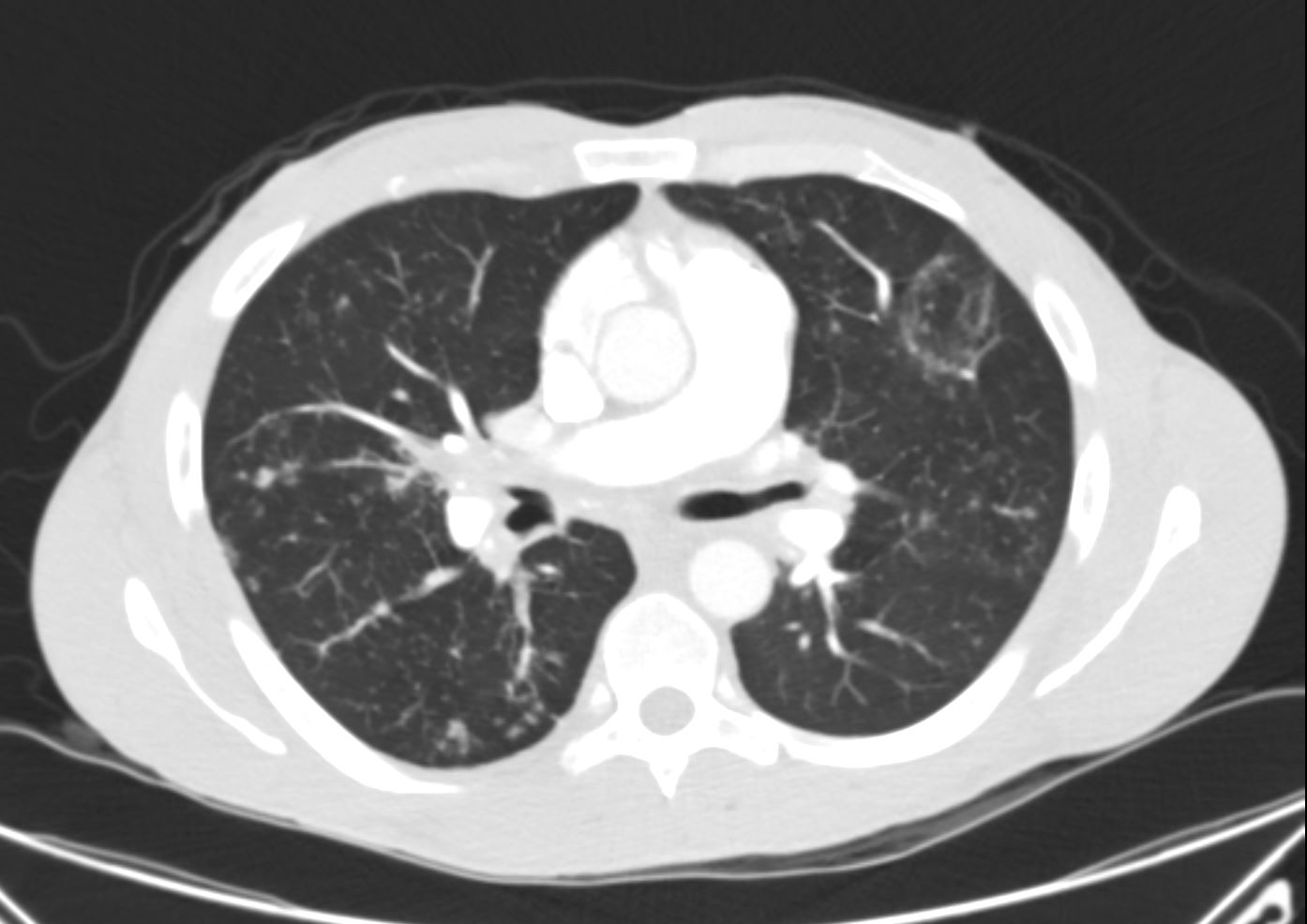
The CT scan, shows diffuse micronodular lung disease, predominantly in the upper lobes with mediastinal widening consistent with mediastinal lymphadenopathy, dominant in the right paratracheal region and in the subcarinal region.
Lung windows show the presence of extensive diffuse micronodular disease accumulating along lymphatics along fissures and pleural surfaces, and along the bronchovascular bundles. Although there is diffuse disease, the upper lobes are slightly more involved than the lower lobes. The extensive thickening along bronchovascular bundles and prominent adenopathy favors a diagnosis of sarcoidosis but with a work history of being a cement worker, silicosis still remains in the differential diagnosis as a less likely possibility.
Ashley Davidoff MDLangerhans Cell Histiocytosis
Ashley Davidoff MD
RETICULONODULAR PATTERN
53-year-old female with nicotine dependence presents with dyspnea and cough
CXR (PA and Lateral) shows bilateral and extensive reticular nodular changes slightly more prominent in the upper lung zones
Ashley Davidoff MD
CT scan from 16 months prior showed multiple relatively thick-walled cysts predominantly in the upper lobes. The cysts are round and air filled large and are between 5mm-8mm
Ashley Davidoff MD